COR Corona COVID-19 forum
Alles over het corona / COVID-19 virus.



Gezien alle fake news en onzin die wordt geplaatst over het Coronavirus, plaats hier alle relevante peer reviewed wetenschappelijke artikelen over Corona (of ook andere artikelen/interviews zolang het door een dokter/wetenschapper is gemaakt). Gelukkig is er veel onderzoek gedaan naar het Coronavirus.
Plaats ook verschillende data analyses/visualisaties en statistieken over het Corona virus.
Actuele informatie en data van het RIVM, dagelijkse update om 14:00
WHO Corona website
Elsevier corona information centre
Coronavirus laatste nieuws van BNO
Aantal bekende grafieken:
Plaats ook verschillende data analyses/visualisaties en statistieken over het Corona virus.
Algemene linkjesquote:SARS-CoV-2, voorheen bekend als 2019-nCoV, is een virus dat de besmettelijke luchtwegaandoening COVID-19 bij mensen veroorzaakt.SARS-CoV-2 is een virus-stam uit het geslacht betacoronavirussen uit de onderfamilie van coronavirussen.
Actuele informatie en data van het RIVM, dagelijkse update om 14:00
WHO Corona website
Elsevier corona information centre
Coronavirus laatste nieuws van BNO

Aantal bekende grafieken:
SPOILEROm spoilers te kunnen lezen moet je zijn ingelogd. Je moet je daarvoor eerst gratis Registreren. Ook kun je spoilers niet lezen als je een ban hebt.Data visualisaties:
https://twitter.com/Datagraver
Voorbeelden:SPOILEROm spoilers te kunnen lezen moet je zijn ingelogd. Je moet je daarvoor eerst gratis Registreren. Ook kun je spoilers niet lezen als je een ban hebt.Worldometer coronavirus site
Mapping the Outbreak timelapse
Preppers kaart verspreiding in NL Nog een kaartje van NL
Nog een kaartje van NL
Wuhan Corona Virus Map
Livetrackers:
(link 1) (link 2) (link 3)
Wetenschappelijke artikelen:
A pneumonia outbreak associated with a new coronavirus of probable bat origin
Coronavirus latest: First vaccine clinical trials begin in United States
China’s response to a novel coronavirus stands in stark contrast to the 2002 SARS outbreak response
Arguments in favor of remdesivir for treating SARS-CoV-2 infections
Chloroquine and hydroxychloroquine as available weapons to fight COVID-19
Coronavirus Disease 2019 (COVID-19): Protecting Hospitals From the Invisible
Clinical features of deaths in the novel coronavirus epidemic in China
COVID‐19 and Rationally Layered Social Distancing
Mental health groups providing support, education in wake of COVID‐19
The potential chemical structure of anti‐SARS‐CoV‐2 RNA‐dependent RNA polymerase
A report of clinical diagnosis and treatment of nine cases of coronavirus disease 2019
2019 novel coronavirus patients’ clinical characteristics, discharge rate and fatality rate of meta‐analysis
Novel Coronavirus (COVID‐19) Epidemic: What Are the Risks for Older Patients?
Plaats gerust artikelen en data en andere verhalen over de mortality rates, comorbidity, comortality, besmettelijkheid, medicijnen, vaccinaties, behandelingen,aanpak van overheden, mentale gezondheid etc. En data visualisaties/analyse en andere statistieken over het Coronavirus. Bij interessante bronnen en nieuws probeer ik de OP te updaten. Deel vooral hier, en zet er altijd even een bron bij. Geen fake news of sensatie nieuws van kranten hier aub
[ Bericht 0% gewijzigd door Momo op 17-03-2020 17:28:48 ]
Also known as Kyran or Theoden
Goed idee. Alleen denk ik dat er te weinig peer reviewed artikelen zullen zijn de komende tijd. Misschien uitbreiden naar ook niet peer reviewed artikelen?
Gewoon een idee
Gewoon een idee
Ja zolang het wetenschappelijke inhoud heeft, kan ook een interview gewoon zijn met een expert.quote:Op dinsdag 17 maart 2020 17:03 schreef Kyran het volgende:
Goed idee. Alleen denk ik dat er te weinig peer reviewed artikelen zullen zijn de komende tijd. Misschien uitbreiden naar ook niet peer reviewed artikelen?
Gewoon een idee
quote:Fosun Pharma and BioNTech form COVID-19 vaccine strategic alliance in China
(15 March 2020, Shanghai, Hong Kong) – Today, Fosun Pharma industrial, a subsidiary company of Shanghai Fosun Pharmaceutical (Group) Co., Ltd (“Fosun Pharma” or “the Group”; Stock Code: 600196.SH, 02196.HK) and BioNTech SE (NASDAQ: BNTX, “BioNTech” or “the Company”) announced a strategic development and commercialization collaboration to advance BioNTech’s mRNA vaccine in China for the prevention of COVID-19 infections.
Under the terms of the agreement, the two Companies will work jointly on the development of COVID-19 vaccines based on BioNTech’s mRNA technology platform in China. The Companies will collaborate to conduct clinical trials in China leveraging Fosun Pharma’s extensive clinical development, regulatory, and commercial capabilities in the country. BioNTech will supply the mRNA vaccine for clinical trials from GMP manufacturing facilities in Europe.
mRNA is a nucleic acid molecule that carries genetic information. The mRNA vaccine introduces the genetic information into the body, so that the cells in the body produce the corresponding antigen, which induces the body to produce neutralizing antibodies and stimulates the response of T cells, and fights against the virus through the dual mechanisms of humoral immunity and cellular immunity. In the face of a sudden epidemic, compared with traditional vaccines, synthesis and production process of mRNA vaccine is more convenient, and has strong immunogenicity, which does not need additional adjuvant as needed by the traditional vaccine, and with good safety.
BioNTech is a leading mRNA technology company that has diversified mRNA platform technologies, integrated R&D system and strong manufacturing capability. “The mRNA technology introduces genetic information into human body, then the body's own cells produce the corresponding proteins that cure or prevent disease. Fosun Pharma R&D has been tracking the development of this technology. The two companies expect further cooperation in this field,” says Dr. Aimin Hui, President of Fosun Pharma Global R&D.
“We see this collaboration as an important step in our global effort to expedite the development of mRNA vaccines to prevent COVID-19 infection. Fosun Pharma shares our commitment to move rapidly to address the COVID-19 outbreak and brings deep development experience and an extensive network in the pharmaceutical market in China,” says Founder and CEO of BioNTech, Ugur Sahin, M.D.
Wu Yifang, President and CEO of Fosun Pharma states, “A potential pandemic requires a collective effort and both companies are passionate about contributing to the fight against the current coronavirus outbreak. We are excited to collaborate with BioNTech, one of the leading companies worldwide in the mRNA field. Our shared objective is to develop a vaccine against the coronavirus and to be able to rapidly manufacture a vaccine to turn the tide of COVID-19 infection.”
Under the terms of the agreement, Fosun Pharma will pay BioNTech up to $85 million in licensing fees (including a down payment, clinical development registration and sales milestone payments) as agreed, and a sales commission equal to 35% of the product's annual gross profit during the agreed sales commission period. Meanwhile, Fosun Pharma has agreed to make an equity investment of USD 50 million (EUR 44 million) for 1,580,777 ordinary shares in BioNTech.
Design of an Epitope-Based Synthetic Long Peptide Vaccine to Counteract the Novel China Coronavirus (2019-nCoV)
In this report, we demonstrate that it is possible to design epitope-based peptide vaccine candidates to counteract the novel China coronavirus (2019-nCoV) by using an approach similar to the one used in cancer neoantigen vaccination therapy. We identified multiepitope peptide vaccine candidates against 2019-nCov that can potentially trigger both CD4+ and CD8+ T cell immune response with increased efficiency due to the presence of CD4+ and CD8+ T cell epitopes and a cathepsin-sensitive linker. Furthermore, we suggest that the peptide design strategy should incorporate population-specific HLA alleles in order to optimize binding specificity of the peptides. We refer to this as populationalized vaccinomics.
In this report, we demonstrate that it is possible to design epitope-based peptide vaccine candidates to counteract the novel China coronavirus (2019-nCoV) by using an approach similar to the one used in cancer neoantigen vaccination therapy. We identified multiepitope peptide vaccine candidates against 2019-nCov that can potentially trigger both CD4+ and CD8+ T cell immune response with increased efficiency due to the presence of CD4+ and CD8+ T cell epitopes and a cathepsin-sensitive linker. Furthermore, we suggest that the peptide design strategy should incorporate population-specific HLA alleles in order to optimize binding specificity of the peptides. We refer to this as populationalized vaccinomics.

Ook even hier een linkje naar het topic van @_I over de verschillende mutaties van Corona virus die nu in de wereld rond gaan. Zo kun je bijvoorbeeld zien dat het Corona virus dat nu vooral actief in de VS vooral uit Azië komt en niet uit Europa. De varianten die je vooral in Nederland vind zijn afkomstig uit Noord-Italië.
Nextstrain
En de website waar dat op staat:
https://nextstrain.org/ncov?c=country&f_country=Japan,USA,China&l=radial
Nextstrain
En de website waar dat op staat:
https://nextstrain.org/ncov?c=country&f_country=Japan,USA,China&l=radial
Zie voorlopig behandeladvies RIVM, en voor behandelopties RIVMquote:
Is al bekend welke onderzoeken het rivm gebruikt?
[ Bericht 0% gewijzigd door Momo op 17-03-2020 19:53:30 ]
https://www.overhetcoronavirus.nl/
arts, klinisch epidemioloog en onderzoeker uit Utrecht die hoofdzakelijk wetenschappelijke bronnen gebruikt.
arts, klinisch epidemioloog en onderzoeker uit Utrecht die hoofdzakelijk wetenschappelijke bronnen gebruikt.
Realiteit is een illusie die ontstaat bij een gebrek aan alcohol
How will country-based mitigation measures influence the course of the COVID-19 epidemic?
Hier ander onderzoek van RIVM onderzoekers in samenwerking met 2 Britse onderzoekers die daar ook in een vergelijkbare rol werken. Ook een beetje in lijn met wat Rutte zei over het verspreiden van besmettingen.
Hier ander onderzoek van RIVM onderzoekers in samenwerking met 2 Britse onderzoekers die daar ook in een vergelijkbare rol werken. Ook een beetje in lijn met wat Rutte zei over het verspreiden van besmettingen.
Ik heb geen verstand van het verloop van mutaties bij virussen. Maar is er ook al iets te zeggen of de verschillende aftakkingen zich anders (bijvoorbeeld agressiever of milder) gedragen? Of is het daar nog te vroeg voor? Of zijn de mutaties die in zo'n korte periode optreden überhaupt niet significant genoeg?quote:
Ook even hier een linkje naar het topic van @:_I over de verschillende mutaties van Corona virus die nu in de wereld rond gaan. Zo kun je bijvoorbeeld zien dat het Corona virus dat nu vooral actief in de VS vooral uit Azië komt en niet uit Europa. De varianten die je vooral in Nederland vind zijn afkomstig uit Noord-Italië.
Nextstrain
En de website waar dat op staat:
https://nextstrain.org/ncov?c=country&f_country=Japan,USA,China&l=radial
Als je naar de sterftecijfers in Italië kijkt dan zou je bijna denken dat daar een meer agressieve variant heerst. Maar dat kan ook hele andere oorzaken hebben (gemiddelde leeftijd van de geïnfecteerden, worden alle besmettingen vastgesteld/geregistreerd, enzovoort).
https://www.globaltimes.cn/content/1181612.shtmlquote:
[..]
Ik heb geen verstand van het verloop van mutaties bij virussen. Maar is er ook al iets te zeggen of de verschillende aftakkingen zich anders (bijvoorbeeld agressiever of milder) gedragen? Of is het daar nog te vroeg voor? Of zijn de mutaties die in zo'n korte periode optreden überhaupt niet significant genoeg?
Als je naar de sterftecijfers in Italië kijkt dan zou je bijna denken dat daar een meer agressieve variant heerst. Maar dat kan ook hele andere oorzaken hebben (gemiddelde leeftijd van de geïnfecteerden, worden alle besmettingen vastgesteld/geregistreerd, enzovoort).
Dat vermoeden is er wel. Waarschijnlijk wordt daar nu meer onderzoek naar gedaan.

Theories of SARS-CoV-2 origins
SPOILEROm spoilers te kunnen lezen moet je zijn ingelogd. Je moet je daarvoor eerst gratis Registreren. Ook kun je spoilers niet lezen als je een ban hebt.Nature

The view from nowhere.
Wat betreft de invloed van temperatuur en vochtigheid op de verspreiding van het virus:
High Temperature and High Humidity Reduce the Transmission of COVID-19
This paper investigates how air temperature and humidity influence the transmission of COVID-19. After estimating the serial interval of COVID-19 from 105 pairs of the virus carrier and the infected, we calculate the daily effective reproductive number, R, for each of all 100 Chinese cities with more than 40 cases. Using the daily R values from January 21 to 23, 2020 as proxies of non-intervened transmission intensity, we find, under a linear regression framework for 100 Chinese cities, high temperature and high relative humidity significantly reduce the transmission of COVID-19, respectively, even after controlling for population density and GDP per capita of cities. One degree Celsius increase in temperature and one percent increase in relative humidity lower R by 0.0383 and 0.0224, respectively. This result is consistent with the fact that the high temperature and high humidity significantly reduce the transmission of influenza. It indicates that the arrival of summer and rainy season in the northern hemisphere can effectively reduce the transmission of the COVID-19.
[ Bericht 5% gewijzigd door Momo op 18-03-2020 10:08:53 ]
High Temperature and High Humidity Reduce the Transmission of COVID-19
This paper investigates how air temperature and humidity influence the transmission of COVID-19. After estimating the serial interval of COVID-19 from 105 pairs of the virus carrier and the infected, we calculate the daily effective reproductive number, R, for each of all 100 Chinese cities with more than 40 cases. Using the daily R values from January 21 to 23, 2020 as proxies of non-intervened transmission intensity, we find, under a linear regression framework for 100 Chinese cities, high temperature and high relative humidity significantly reduce the transmission of COVID-19, respectively, even after controlling for population density and GDP per capita of cities. One degree Celsius increase in temperature and one percent increase in relative humidity lower R by 0.0383 and 0.0224, respectively. This result is consistent with the fact that the high temperature and high humidity significantly reduce the transmission of influenza. It indicates that the arrival of summer and rainy season in the northern hemisphere can effectively reduce the transmission of the COVID-19.
[ Bericht 5% gewijzigd door Momo op 18-03-2020 10:08:53 ]
Aerosol and Surface Stability of SARS-CoV-2 as Compared with SARS-CoV-1
A novel human coronavirus that is now named severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) (formerly called HCoV-19) emerged in Wuhan, China, in late 2019 and is now causing a pandemic.1 We analyzed the aerosol and surface stability of SARS-CoV-2 and compared it with SARS-CoV-1, the most closely related human coronavirus.2
We evaluated the stability of SARS-CoV-2 and SARS-CoV-1 in aerosols and on various surfaces and estimated their decay rates using a Bayesian regression model (see the Methods section in the Supplementary Appendix, available with the full text of this letter at NEJM.org). SARS-CoV-2 nCoV-WA1-2020 (MN985325.1) and SARS-CoV-1 Tor2 (AY274119.3) were the strains used. Aerosols (<5 μm) containing SARS-CoV-2 (105.25 50% tissue-culture infectious dose [TCID50] per milliliter) or SARS-CoV-1 (106.75-7.00 TCID50 per milliliter) were generated with the use of a three-jet Collison nebulizer and fed into a Goldberg drum to create an aerosolized environment. The inoculum resulted in cycle-threshold values between 20 and 22, similar to those observed in samples obtained from the upper and lower respiratory tract in humans.
Our data consisted of 10 experimental conditions involving two viruses (SARS-CoV-2 and SARS-CoV-1) in five environmental conditions (aerosols, plastic, stainless steel, copper, and cardboard). All experimental measurements are reported as means across three replicates.
SARS-CoV-2 remained viable in aerosols throughout the duration of our experiment (3 hours), with a reduction in infectious titer from 103.5 to 102.7 TCID50 per liter of air. This reduction was similar to that observed with SARS-CoV-1, from 104.3 to 103.5 TCID50 per milliliter (Figure 1A).
SARS-CoV-2 was more stable on plastic and stainless steel than on copper and cardboard, and viable virus was detected up to 72 hours after application to these surfaces (Figure 1A), although the virus titer was greatly reduced (from 103.7 to 100.6 TCID50 per milliliter of medium after 72 hours on plastic and from 103.7 to 100.6 TCID50 per milliliter after 48 hours on stainless steel). The stability kinetics of SARS-CoV-1 were similar (from 103.4 to 100.7 TCID50 per milliliter after 72 hours on plastic and from 103.6 to 100.6 TCID50 per milliliter after 48 hours on stainless steel). On copper, no viable SARS-CoV-2 was measured after 4 hours and no viable SARS-CoV-1 was measured after 8 hours. On cardboard, no viable SARS-CoV-2 was measured after 24 hours and no viable SARS-CoV-1 was measured after 8 hours (Figure 1A).
Both viruses had an exponential decay in virus titer across all experimental conditions, as indicated by a linear decrease in the log10TCID50 per liter of air or milliliter of medium over time (Figure 1B). The half-lives of SARS-CoV-2 and SARS-CoV-1 were similar in aerosols, with median estimates of approximately 1.1 to 1.2 hours and 95% credible intervals of 0.64 to 2.64 for SARS-CoV-2 and 0.78 to 2.43 for SARS-CoV-1 (Figure 1C, and Table S1 in the Supplementary Appendix). The half-lives of the two viruses were also similar on copper. On cardboard, the half-life of SARS-CoV-2 was longer than that of SARS-CoV-1. The longest viability of both viruses was on stainless steel and plastic; the estimated median half-life of SARS-CoV-2 was approximately 5.6 hours on stainless steel and 6.8 hours on plastic (Figure 1C). Estimated differences in the half-lives of the two viruses were small except for those on cardboard (Figure 1C). Individual replicate data were noticeably “noisier” (i.e., there was more variation in the experiment, resulting in a larger standard error) for cardboard than for other surfaces (Fig. S1 through S5), so we advise caution in interpreting this result.
We found that the stability of SARS-CoV-2 was similar to that of SARS-CoV-1 under the experimental circumstances tested. This indicates that differences in the epidemiologic characteristics of these viruses probably arise from other factors, including high viral loads in the upper respiratory tract and the potential for persons infected with SARS-CoV-2 to shed and transmit the virus while asymptomatic.3,4 Our results indicate that aerosol and fomite transmission of SARS-CoV-2 is plausible, since the virus can remain viable and infectious in aerosols for hours and on surfaces up to days (depending on the inoculum shed). These findings echo those with SARS-CoV-1, in which these forms of transmission were associated with nosocomial spread and super-spreading events,5 and they provide information for pandemic mitigation efforts.
A novel human coronavirus that is now named severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) (formerly called HCoV-19) emerged in Wuhan, China, in late 2019 and is now causing a pandemic.1 We analyzed the aerosol and surface stability of SARS-CoV-2 and compared it with SARS-CoV-1, the most closely related human coronavirus.2
We evaluated the stability of SARS-CoV-2 and SARS-CoV-1 in aerosols and on various surfaces and estimated their decay rates using a Bayesian regression model (see the Methods section in the Supplementary Appendix, available with the full text of this letter at NEJM.org). SARS-CoV-2 nCoV-WA1-2020 (MN985325.1) and SARS-CoV-1 Tor2 (AY274119.3) were the strains used. Aerosols (<5 μm) containing SARS-CoV-2 (105.25 50% tissue-culture infectious dose [TCID50] per milliliter) or SARS-CoV-1 (106.75-7.00 TCID50 per milliliter) were generated with the use of a three-jet Collison nebulizer and fed into a Goldberg drum to create an aerosolized environment. The inoculum resulted in cycle-threshold values between 20 and 22, similar to those observed in samples obtained from the upper and lower respiratory tract in humans.
Our data consisted of 10 experimental conditions involving two viruses (SARS-CoV-2 and SARS-CoV-1) in five environmental conditions (aerosols, plastic, stainless steel, copper, and cardboard). All experimental measurements are reported as means across three replicates.
SARS-CoV-2 remained viable in aerosols throughout the duration of our experiment (3 hours), with a reduction in infectious titer from 103.5 to 102.7 TCID50 per liter of air. This reduction was similar to that observed with SARS-CoV-1, from 104.3 to 103.5 TCID50 per milliliter (Figure 1A).
SARS-CoV-2 was more stable on plastic and stainless steel than on copper and cardboard, and viable virus was detected up to 72 hours after application to these surfaces (Figure 1A), although the virus titer was greatly reduced (from 103.7 to 100.6 TCID50 per milliliter of medium after 72 hours on plastic and from 103.7 to 100.6 TCID50 per milliliter after 48 hours on stainless steel). The stability kinetics of SARS-CoV-1 were similar (from 103.4 to 100.7 TCID50 per milliliter after 72 hours on plastic and from 103.6 to 100.6 TCID50 per milliliter after 48 hours on stainless steel). On copper, no viable SARS-CoV-2 was measured after 4 hours and no viable SARS-CoV-1 was measured after 8 hours. On cardboard, no viable SARS-CoV-2 was measured after 24 hours and no viable SARS-CoV-1 was measured after 8 hours (Figure 1A).
Both viruses had an exponential decay in virus titer across all experimental conditions, as indicated by a linear decrease in the log10TCID50 per liter of air or milliliter of medium over time (Figure 1B). The half-lives of SARS-CoV-2 and SARS-CoV-1 were similar in aerosols, with median estimates of approximately 1.1 to 1.2 hours and 95% credible intervals of 0.64 to 2.64 for SARS-CoV-2 and 0.78 to 2.43 for SARS-CoV-1 (Figure 1C, and Table S1 in the Supplementary Appendix). The half-lives of the two viruses were also similar on copper. On cardboard, the half-life of SARS-CoV-2 was longer than that of SARS-CoV-1. The longest viability of both viruses was on stainless steel and plastic; the estimated median half-life of SARS-CoV-2 was approximately 5.6 hours on stainless steel and 6.8 hours on plastic (Figure 1C). Estimated differences in the half-lives of the two viruses were small except for those on cardboard (Figure 1C). Individual replicate data were noticeably “noisier” (i.e., there was more variation in the experiment, resulting in a larger standard error) for cardboard than for other surfaces (Fig. S1 through S5), so we advise caution in interpreting this result.
We found that the stability of SARS-CoV-2 was similar to that of SARS-CoV-1 under the experimental circumstances tested. This indicates that differences in the epidemiologic characteristics of these viruses probably arise from other factors, including high viral loads in the upper respiratory tract and the potential for persons infected with SARS-CoV-2 to shed and transmit the virus while asymptomatic.3,4 Our results indicate that aerosol and fomite transmission of SARS-CoV-2 is plausible, since the virus can remain viable and infectious in aerosols for hours and on surfaces up to days (depending on the inoculum shed). These findings echo those with SARS-CoV-1, in which these forms of transmission were associated with nosocomial spread and super-spreading events,5 and they provide information for pandemic mitigation efforts.

Dit is niet best toch, kan je dus in je tuin het oplopen van iemand straten verderop etc. Nachtmerriequote:
Aerosol and Surface Stability of SARS-CoV-2 as Compared with SARS-CoV-1
A novel human coronavirus that is now named severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) (formerly called HCoV-19) emerged in Wuhan, China, in late 2019 and is now causing a pandemic.1 We analyzed the aerosol and surface stability of SARS-CoV-2 and compared it with SARS-CoV-1, the most closely related human coronavirus.2
We evaluated the stability of SARS-CoV-2 and SARS-CoV-1 in aerosols and on various surfaces and estimated their decay rates using a Bayesian regression model (see the Methods section in the Supplementary Appendix, available with the full text of this letter at NEJM.org). SARS-CoV-2 nCoV-WA1-2020 (MN985325.1) and SARS-CoV-1 Tor2 (AY274119.3) were the strains used. Aerosols (<5 μm) containing SARS-CoV-2 (105.25 50% tissue-culture infectious dose [TCID50] per milliliter) or SARS-CoV-1 (106.75-7.00 TCID50 per milliliter) were generated with the use of a three-jet Collison nebulizer and fed into a Goldberg drum to create an aerosolized environment. The inoculum resulted in cycle-threshold values between 20 and 22, similar to those observed in samples obtained from the upper and lower respiratory tract in humans.
Our data consisted of 10 experimental conditions involving two viruses (SARS-CoV-2 and SARS-CoV-1) in five environmental conditions (aerosols, plastic, stainless steel, copper, and cardboard). All experimental measurements are reported as means across three replicates.
SARS-CoV-2 remained viable in aerosols throughout the duration of our experiment (3 hours), with a reduction in infectious titer from 103.5 to 102.7 TCID50 per liter of air. This reduction was similar to that observed with SARS-CoV-1, from 104.3 to 103.5 TCID50 per milliliter (Figure 1A).
SARS-CoV-2 was more stable on plastic and stainless steel than on copper and cardboard, and viable virus was detected up to 72 hours after application to these surfaces (Figure 1A), although the virus titer was greatly reduced (from 103.7 to 100.6 TCID50 per milliliter of medium after 72 hours on plastic and from 103.7 to 100.6 TCID50 per milliliter after 48 hours on stainless steel). The stability kinetics of SARS-CoV-1 were similar (from 103.4 to 100.7 TCID50 per milliliter after 72 hours on plastic and from 103.6 to 100.6 TCID50 per milliliter after 48 hours on stainless steel). On copper, no viable SARS-CoV-2 was measured after 4 hours and no viable SARS-CoV-1 was measured after 8 hours. On cardboard, no viable SARS-CoV-2 was measured after 24 hours and no viable SARS-CoV-1 was measured after 8 hours (Figure 1A).
Both viruses had an exponential decay in virus titer across all experimental conditions, as indicated by a linear decrease in the log10TCID50 per liter of air or milliliter of medium over time (Figure 1B). The half-lives of SARS-CoV-2 and SARS-CoV-1 were similar in aerosols, with median estimates of approximately 1.1 to 1.2 hours and 95% credible intervals of 0.64 to 2.64 for SARS-CoV-2 and 0.78 to 2.43 for SARS-CoV-1 (Figure 1C, and Table S1 in the Supplementary Appendix). The half-lives of the two viruses were also similar on copper. On cardboard, the half-life of SARS-CoV-2 was longer than that of SARS-CoV-1. The longest viability of both viruses was on stainless steel and plastic; the estimated median half-life of SARS-CoV-2 was approximately 5.6 hours on stainless steel and 6.8 hours on plastic (Figure 1C). Estimated differences in the half-lives of the two viruses were small except for those on cardboard (Figure 1C). Individual replicate data were noticeably “noisier” (i.e., there was more variation in the experiment, resulting in a larger standard error) for cardboard than for other surfaces (Fig. S1 through S5), so we advise caution in interpreting this result.
We found that the stability of SARS-CoV-2 was similar to that of SARS-CoV-1 under the experimental circumstances tested. This indicates that differences in the epidemiologic characteristics of these viruses probably arise from other factors, including high viral loads in the upper respiratory tract and the potential for persons infected with SARS-CoV-2 to shed and transmit the virus while asymptomatic.3,4 Our results indicate that aerosol and fomite transmission of SARS-CoV-2 is plausible, since the virus can remain viable and infectious in aerosols for hours and on surfaces up to days (depending on the inoculum shed). These findings echo those with SARS-CoV-1, in which these forms of transmission were associated with nosocomial spread and super-spreading events,5 and they provide information for pandemic mitigation efforts.
[ afbeelding ]
Mutations can reveal how the coronavirus moves—but they’re easy to overinterpret
mmediately after Christian Drosten published a genetic sequence of the novel coronavirus online on 28 February, he took to Twitter to issue a warning. As the virus has raced around the world, more than 350 genome sequences have been shared on the online platform GISAID. They hold clues to how the new virus, named severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), is spreading and evolving. But because the sequences represent a tiny fraction of cases and show few telltale differences, they are easy to overinterpret, as Drosten realized.
A virologist at the Charité University Hospital in Berlin, he had sequenced the virus from a German patient infected with COVID-19 in Italy. The genome looked similar to that of a virus found in a patient in Munich, the capital of Bavaria, more than 1 month earlier; both shared three mutations not seen in early sequences from China. Drosten realized this could give rise to the idea that the Italian outbreak was “seeded” by the one in Bavaria, which state public health officials said had been quashed by tracing and quarantining all contacts of the 14 confirmed cases. But he thought it was just as likely that a Chinese variant carrying the three mutations had taken independent routes to both countries. The newly sequenced genome “is not sufficient to claim a link between Munich and Italy,” Drosten tweeted.
His warning went unheeded. A few days later, Trevor Bedford of the Fred Hutchinson Cancer Research Center, who analyzes the stream of viral genomes and discusses them in Twitter threads, wrote that the pattern suggested the outbreak in Bavaria had not been contained after all, and appeared to have led to the Italian outbreak. The analysis spread widely. Technology Review asserted that “the Munich event could be linked to a decent part of the overall European outbreak” and Twitter users called on Germany to apologize. (This Science correspondent retweeted Bedford’s thread as well.)
irologist Eeva Broberg of the European Centre for Disease Prevention and Control agrees with Drosten that there are more plausible scenarios for how the disease reached northern Italy than an undetected spread from Bavaria. Other scientists say Bedford jumped the gun as well. “I have to kick his butt a bit for this,” says Richard Neher, a computational biologist at the University of Basel who works with Bedford. “It’s a cautionary tale,” says Andrew Rambaut, a molecular evolutionary biologist at the University of Edinburgh. “There is no way you can make that claim just from the phylogeny alone.” Bedford later clarified he believed it was equally plausible there had been two separate introductions from China. “I think I should have been more careful with that Twitter thread,” he says.
It was a case study in the power and pitfalls of real-time analysis of viral genomes. “This is an incredibly important disease. We need to understand how it is moving,” says Bette Korber, a biologist at Los Alamos National Laboratory who is also studying the genome of SARS-CoV-2. “With very limited evolution during the outbreak, [these researchers] are doing what they can and they are making suggestions, which I think at this point should be taken as suggestions.”
The sequence data were most informative early on, says Kristian Andersen, a computational biologist at Scripps Research. The very first sequence, in early January, answered the most basic question: What pathogen is causing the disease? The ones that followed were almost identical, strongly suggesting there was a single introduction from an animal into the human population. If the virus had jumped the species barrier multiple times, scientists would see more variety among the first human cases.
Now, more diversity is emerging. Like all viruses, SARS-CoV-2 evolves over time through random mutations, only some of which are caught and corrected by the virus’s error correction machinery. Over the length of its 30,000-base-pair genome, SARS-CoV-2 accumulates an average of about one to two mutations per month, Rambaut says. “It’s about two to four times slower than the flu,” he says. Using these little changes, researchers can draw up phylogenetic trees, much like family trees. They can also make connections between different cases of COVID-19 and gauge whether there might be undetected spread of the virus.
For instance, when researchers sequenced the second virus genome in Washington—from a teenager diagnosed with COVID-19 on 27 February—it looked like a direct descendant of the first genome, a case found 6 weeks earlier, that had acquired three further mutations. Bedford tweeted that he considered it “highly unlikely” that the two genomes came from separate introductions. “I believe we are facing an already substantial outbreak in Washington State that was not detected until now,” he wrote. That analysis turned out to be correct: Washington has now reported more than 100 cases and 15 deaths and additional genomes from other patients have bolstered the link. In this case, Bedford’s hypothesis was much stronger because the two patients both came from Snohomish County, Rambaut says: “It’s very unlikely that this highly related virus would travel to exactly the same town in Washington,” he says.
Few other firm conclusions about the virus’s spread have emerged, in part because the wealth of genomes is still a tiny sample of the more than 100,000 cases worldwide. Although China accounts for 80% of all COVID-19 cases, only one-third of the published genomes are from China—and very few of them are from later cases. And because it’s early in the outbreak, most genomes are still very similar, which makes it hard to draw conclusions. “We just have this handful of mutations, which makes these groupings so ambiguous,” Neher says. “As the outbreak unfolds, we expect to see more and more diversity and more clearly distinct lineages,” he says. “And then it will become easier and easier to actually put things together.”
Scientists will also be scouring the genomic diversity for mutations that might change how dangerous the pathogen is or how fast it spreads. There, too, caution is warranted. A paper published by Lu Jian of Peking University and colleagues on 3 March in the journal National Science Review analyzed 103 virus genomes and argued that they fell into one of two distinct types, named S and L, distinguished by two mutations. Because 70% of sequenced SARS-CoV-2 genomes belong to L, the newer type, the authors concluded that virus has evolved to become more aggressive and to spread faster.
But they lack evidence, Rambaut says. “What they’ve done is basically seen these two branches and said, ‘That one is bigger, [so that virus] must be more virulent or more transmissible,’” he says. However, just because a virus is exported and leads to a large outbreak elsewhere does not mean it is behaving differently: “One of these lineages is going to be bigger than the other just by chance.” Some researchers have called for the paper to be retracted. “The claims made in it are clearly unfounded and risk spreading dangerous misinformation at a crucial time in the outbreak,” four scientists at the University of Glasgow wrote in a response published on www.virological.org. (In a response, Lu wrote the four had misunderstood his study.)
Most genomic changes don’t alter the virus’s behavior, Drosten says. The only way to confirm that a mutation has an effect is to study it in cell cultures or animal models and show, for instance, that it has become better at entering cells or transmitting, he says. And if the virus does change in an important way, it could go either way, making it more or less dangerous. In 2018, Drosten’s group published a paper showing that early in the SARS outbreak of 2002–03, that virus lost a small chunk of its genome, 29 base pairs in one gene. Adding those base pairs back in the lab made the virus much better at replicating in several cell culture models.
It might seem strange that a mutation that weakens the virus would become established, but that can happen when it has just entered the human population and isn’t competing with strains lacking the mutation, Drosten says. “Sadly, this new virus doesn’t have that deletion,” he adds
mmediately after Christian Drosten published a genetic sequence of the novel coronavirus online on 28 February, he took to Twitter to issue a warning. As the virus has raced around the world, more than 350 genome sequences have been shared on the online platform GISAID. They hold clues to how the new virus, named severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), is spreading and evolving. But because the sequences represent a tiny fraction of cases and show few telltale differences, they are easy to overinterpret, as Drosten realized.
A virologist at the Charité University Hospital in Berlin, he had sequenced the virus from a German patient infected with COVID-19 in Italy. The genome looked similar to that of a virus found in a patient in Munich, the capital of Bavaria, more than 1 month earlier; both shared three mutations not seen in early sequences from China. Drosten realized this could give rise to the idea that the Italian outbreak was “seeded” by the one in Bavaria, which state public health officials said had been quashed by tracing and quarantining all contacts of the 14 confirmed cases. But he thought it was just as likely that a Chinese variant carrying the three mutations had taken independent routes to both countries. The newly sequenced genome “is not sufficient to claim a link between Munich and Italy,” Drosten tweeted.
His warning went unheeded. A few days later, Trevor Bedford of the Fred Hutchinson Cancer Research Center, who analyzes the stream of viral genomes and discusses them in Twitter threads, wrote that the pattern suggested the outbreak in Bavaria had not been contained after all, and appeared to have led to the Italian outbreak. The analysis spread widely. Technology Review asserted that “the Munich event could be linked to a decent part of the overall European outbreak” and Twitter users called on Germany to apologize. (This Science correspondent retweeted Bedford’s thread as well.)
irologist Eeva Broberg of the European Centre for Disease Prevention and Control agrees with Drosten that there are more plausible scenarios for how the disease reached northern Italy than an undetected spread from Bavaria. Other scientists say Bedford jumped the gun as well. “I have to kick his butt a bit for this,” says Richard Neher, a computational biologist at the University of Basel who works with Bedford. “It’s a cautionary tale,” says Andrew Rambaut, a molecular evolutionary biologist at the University of Edinburgh. “There is no way you can make that claim just from the phylogeny alone.” Bedford later clarified he believed it was equally plausible there had been two separate introductions from China. “I think I should have been more careful with that Twitter thread,” he says.
It was a case study in the power and pitfalls of real-time analysis of viral genomes. “This is an incredibly important disease. We need to understand how it is moving,” says Bette Korber, a biologist at Los Alamos National Laboratory who is also studying the genome of SARS-CoV-2. “With very limited evolution during the outbreak, [these researchers] are doing what they can and they are making suggestions, which I think at this point should be taken as suggestions.”
The sequence data were most informative early on, says Kristian Andersen, a computational biologist at Scripps Research. The very first sequence, in early January, answered the most basic question: What pathogen is causing the disease? The ones that followed were almost identical, strongly suggesting there was a single introduction from an animal into the human population. If the virus had jumped the species barrier multiple times, scientists would see more variety among the first human cases.
Now, more diversity is emerging. Like all viruses, SARS-CoV-2 evolves over time through random mutations, only some of which are caught and corrected by the virus’s error correction machinery. Over the length of its 30,000-base-pair genome, SARS-CoV-2 accumulates an average of about one to two mutations per month, Rambaut says. “It’s about two to four times slower than the flu,” he says. Using these little changes, researchers can draw up phylogenetic trees, much like family trees. They can also make connections between different cases of COVID-19 and gauge whether there might be undetected spread of the virus.
For instance, when researchers sequenced the second virus genome in Washington—from a teenager diagnosed with COVID-19 on 27 February—it looked like a direct descendant of the first genome, a case found 6 weeks earlier, that had acquired three further mutations. Bedford tweeted that he considered it “highly unlikely” that the two genomes came from separate introductions. “I believe we are facing an already substantial outbreak in Washington State that was not detected until now,” he wrote. That analysis turned out to be correct: Washington has now reported more than 100 cases and 15 deaths and additional genomes from other patients have bolstered the link. In this case, Bedford’s hypothesis was much stronger because the two patients both came from Snohomish County, Rambaut says: “It’s very unlikely that this highly related virus would travel to exactly the same town in Washington,” he says.
Few other firm conclusions about the virus’s spread have emerged, in part because the wealth of genomes is still a tiny sample of the more than 100,000 cases worldwide. Although China accounts for 80% of all COVID-19 cases, only one-third of the published genomes are from China—and very few of them are from later cases. And because it’s early in the outbreak, most genomes are still very similar, which makes it hard to draw conclusions. “We just have this handful of mutations, which makes these groupings so ambiguous,” Neher says. “As the outbreak unfolds, we expect to see more and more diversity and more clearly distinct lineages,” he says. “And then it will become easier and easier to actually put things together.”
Scientists will also be scouring the genomic diversity for mutations that might change how dangerous the pathogen is or how fast it spreads. There, too, caution is warranted. A paper published by Lu Jian of Peking University and colleagues on 3 March in the journal National Science Review analyzed 103 virus genomes and argued that they fell into one of two distinct types, named S and L, distinguished by two mutations. Because 70% of sequenced SARS-CoV-2 genomes belong to L, the newer type, the authors concluded that virus has evolved to become more aggressive and to spread faster.
But they lack evidence, Rambaut says. “What they’ve done is basically seen these two branches and said, ‘That one is bigger, [so that virus] must be more virulent or more transmissible,’” he says. However, just because a virus is exported and leads to a large outbreak elsewhere does not mean it is behaving differently: “One of these lineages is going to be bigger than the other just by chance.” Some researchers have called for the paper to be retracted. “The claims made in it are clearly unfounded and risk spreading dangerous misinformation at a crucial time in the outbreak,” four scientists at the University of Glasgow wrote in a response published on www.virological.org. (In a response, Lu wrote the four had misunderstood his study.)
Most genomic changes don’t alter the virus’s behavior, Drosten says. The only way to confirm that a mutation has an effect is to study it in cell cultures or animal models and show, for instance, that it has become better at entering cells or transmitting, he says. And if the virus does change in an important way, it could go either way, making it more or less dangerous. In 2018, Drosten’s group published a paper showing that early in the SARS outbreak of 2002–03, that virus lost a small chunk of its genome, 29 base pairs in one gene. Adding those base pairs back in the lab made the virus much better at replicating in several cell culture models.
It might seem strange that a mutation that weakens the virus would become established, but that can happen when it has just entered the human population and isn’t competing with strains lacking the mutation, Drosten says. “Sadly, this new virus doesn’t have that deletion,” he adds
COVID-19 coronavirus epidemic has a natural origin
The novel SARS-CoV-2 coronavirus that emerged in the city of Wuhan, China, last year and has since caused a large scale COVID-19 epidemic and spread to more than 70 other countries is the product of natural evolution, according to findings published today in the journal Nature Medicine.
Kristian G. Andersen, Andrew Rambaut, W. Ian Lipkin, Edward C. Holmes, Robert F. Garry. The proximal origin of SARS-CoV-2. Nature Medicine, 2020; DOI: 10.1038/s41591-020-0820-9
Median incubation period for COVID-19
A new study calculates that the median incubation period for COVID-19 is just over 5 days and that 97.5% of people who develop symptoms will do so within 11.5 days of infection.
Stephen A. Lauer, Kyra H. Grantz, Qifang Bi, Forrest K. Jones, Qulu Zheng, Hannah R. Meredith, Andrew S. Azman, Nicholas G. Reich, Justin Lessler. The Incubation Period of Coronavirus Disease 2019 (COVID-19) From Publicly Reported Confirmed Cases: Estimation and Application. Annals of Internal Medicine, 2020; DOI: 10.7326/M20-0504
New coronavirus stable for hours on surfaces
Ah die stond al hierboven zie ik.
The novel SARS-CoV-2 coronavirus that emerged in the city of Wuhan, China, last year and has since caused a large scale COVID-19 epidemic and spread to more than 70 other countries is the product of natural evolution, according to findings published today in the journal Nature Medicine.
Kristian G. Andersen, Andrew Rambaut, W. Ian Lipkin, Edward C. Holmes, Robert F. Garry. The proximal origin of SARS-CoV-2. Nature Medicine, 2020; DOI: 10.1038/s41591-020-0820-9
Median incubation period for COVID-19
A new study calculates that the median incubation period for COVID-19 is just over 5 days and that 97.5% of people who develop symptoms will do so within 11.5 days of infection.
Stephen A. Lauer, Kyra H. Grantz, Qifang Bi, Forrest K. Jones, Qulu Zheng, Hannah R. Meredith, Andrew S. Azman, Nicholas G. Reich, Justin Lessler. The Incubation Period of Coronavirus Disease 2019 (COVID-19) From Publicly Reported Confirmed Cases: Estimation and Application. Annals of Internal Medicine, 2020; DOI: 10.7326/M20-0504
New coronavirus stable for hours on surfaces
Ah die stond al hierboven zie ik.
New kind of CRISPR technology to target RNA, including RNA viruses like coronavirus
Type VI CRISPR enzymes are RNA-targeting proteins with nuclease activity that enable specific and robust target gene knockdown without altering the genome. To define rules for the design of Cas13d guide RNAs (gRNAs), we conducted massively parallel screens targeting messenger RNAs (mRNAs) of a green fluorescent protein transgene, and CD46, CD55 and CD71 cell-surface proteins in human cells. In total, we measured the activity of 24,460 gRNAs with and without mismatches relative to the target sequences. Knockdown efficacy is driven by gRNA-specific features and target site context. Single mismatches generally reduce knockdown to a modest degree, but spacer nucleotides 15–21 are largely intolerant of target site mismatches. We developed a computational model to identify optimal gRNAs and confirm their generalizability, testing 3,979 guides targeting mRNAs of 48 endogenous genes. We show that Cas13 can be used in forward transcriptomic pooled screens and, using our model, predict optimized Cas13 gRNAs for all protein-coding transcripts in the human genome.
Type VI CRISPR enzymes are RNA-targeting proteins with nuclease activity that enable specific and robust target gene knockdown without altering the genome. To define rules for the design of Cas13d guide RNAs (gRNAs), we conducted massively parallel screens targeting messenger RNAs (mRNAs) of a green fluorescent protein transgene, and CD46, CD55 and CD71 cell-surface proteins in human cells. In total, we measured the activity of 24,460 gRNAs with and without mismatches relative to the target sequences. Knockdown efficacy is driven by gRNA-specific features and target site context. Single mismatches generally reduce knockdown to a modest degree, but spacer nucleotides 15–21 are largely intolerant of target site mismatches. We developed a computational model to identify optimal gRNAs and confirm their generalizability, testing 3,979 guides targeting mRNAs of 48 endogenous genes. We show that Cas13 can be used in forward transcriptomic pooled screens and, using our model, predict optimized Cas13 gRNAs for all protein-coding transcripts in the human genome.
Zit net de persconferentie van de WHO te kijken. Hier kwam de vraag ook voorbij over waarom het sterftecijfer in Italië zo hoog is. Redenen die genoemd werden:quote:
[..]
https://www.globaltimes.cn/content/1181612.shtml
Dat vermoeden is er wel. Waarschijnlijk wordt daar nu meer onderzoek naar gedaan.
* Mate van testen: hoe meer er getest wordt, hoe lager het sterftepercentage
* Leeftijdsdistributie van de besmette bevolking. In Italië ligt die hoger dan bij bijvoorbeeld de besmettingsgroep in Korea.
* Italië zit momenteel verder in de verspreidingscyclus. Sommige patiënten liggen eerst een aantal weken op de IC en overlijden dan alsnog. Die cijfers komen dus pas op een veel later moment in de cijfers terecht.
* De mate waarin de IC's het aantal opnames aankan. In Italië zijn in sommige regio's de IC's overspoeld, wat tot meer doden leidt.
Er werd (gelukkig) nog niks genoemd over een mogelijk agressievere mutatie.


Een heel stuk over besmetten zonder dat je symptomen hebt:
Presumed Asymptomatic Carrier Transmission of COVID-19
A novel coronavirus has resulted in an ongoing outbreak of viral pneumonia in China.1-3 Person-to-person transmission has been demonstrated,1 but, to our knowledge, transmission of the novel coronavirus that causes coronavirus disease 2019 (COVID-19) from an asymptomatic carrier with normal chest computed tomography (CT) findings has not been reported.
Presumed Asymptomatic Carrier Transmission of COVID-19
A novel coronavirus has resulted in an ongoing outbreak of viral pneumonia in China.1-3 Person-to-person transmission has been demonstrated,1 but, to our knowledge, transmission of the novel coronavirus that causes coronavirus disease 2019 (COVID-19) from an asymptomatic carrier with normal chest computed tomography (CT) findings has not been reported.
Deze past hier denk ik ook wel:
quote:
Ik probeer het nog één keer zo nadat mijn topic gesloten werd.
Chinees ziekenhuis heeft hun bevindingen omtrent corona virus op papier gezet. vooral gericht op medisch personeel maar heel interessant om te lezen. Zou eigenlijk onder al het personeel in ziekenhuis verspreid moeten worden.
Via onderstaande link te downloaden.
https://covid-19.alibabacloud.com
Wer lesen kann, ist klar im Vorteil.
Over het ontwikkelen van PTSS na het beleven van Covid-19 infectie zelf of in je omgeving:
Prevalence and predictors of PTSS during COVID-19 Outbreak in China Hardest-hit Areas: Gender differences matter
Highlights
•The prevalence of posttraumatic stress symptoms (PTSS) in China hardest-hit areas a month after the COVID-19 outbreak was 7%.
•Hierarchical regression analysis and non-parametric test suggested that women reported significant higher PTSS in the domains of re-experiencing, negative alterations in cognition or mood, and hyper-arousal.
•Participants with better sleep quality or less frequency of early awakenings reported lower PTSS.
Prevalence and predictors of PTSS during COVID-19 Outbreak in China Hardest-hit Areas: Gender differences matter
Highlights
•The prevalence of posttraumatic stress symptoms (PTSS) in China hardest-hit areas a month after the COVID-19 outbreak was 7%.
•Hierarchical regression analysis and non-parametric test suggested that women reported significant higher PTSS in the domains of re-experiencing, negative alterations in cognition or mood, and hyper-arousal.
•Participants with better sleep quality or less frequency of early awakenings reported lower PTSS.
Geupdate versie van klinische beschrijving van 69 patienten in China
Clinical Features of 69 Cases with Coronavirus Disease 2019 in Wuhan, China
From December 2019 to February 2020, 2019 severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has caused a serious outbreak of coronavirus disease 2019 (COVID-19) in Wuhan, China. Related clinical features are needed.
We reviewed 69 patients who were hospitalized in Union hospital in Wuhan between January 16 to January 29, 2020. All patients were confirmed to be infected with SARS-CoV-2 and the final date of follow-up was February 4, 2020.
The median age of 69 enrolled patients was 42.0 years (IQR 35.0-62.0), and 32 patients (46%) were men. The most common symptoms were fever (60[87%]), cough (38[55%]), and fatigue (29[42%]). Most patients received antiviral therapy (66 [98.5%] of 67 patients) and antibiotic therapy (66 [98.5%] of 67 patients). As of February 4, 2020, 18 (26.9%) of 67 patients had been discharged, and five patients had died, with a mortality rate of 7.5%. According to the lowest SpO2 during admission, cases were divided into the SpO2≥90% group (n=55) and the SpO2<90% group (n=14). All 5 deaths occurred in the SpO2<90% group. Compared with SpO2≥90% group, patients of the SpO2<90% group were older, and showed more comorbidities and higher plasma levels of IL6, IL10, lactate dehydrogenase, and c reactive protein. Arbidol treatment showed tendency to improve the discharging rate and decrease the mortality rate.
COVID-19 appears to show frequent fever, dry cough, and increase of inflammatory cytokines, and induced a mortality rate of 7.5%. Older patients or those with underlying comorbidities are at higher risk of death.
Clinical Features of 69 Cases with Coronavirus Disease 2019 in Wuhan, China
From December 2019 to February 2020, 2019 severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has caused a serious outbreak of coronavirus disease 2019 (COVID-19) in Wuhan, China. Related clinical features are needed.
We reviewed 69 patients who were hospitalized in Union hospital in Wuhan between January 16 to January 29, 2020. All patients were confirmed to be infected with SARS-CoV-2 and the final date of follow-up was February 4, 2020.
The median age of 69 enrolled patients was 42.0 years (IQR 35.0-62.0), and 32 patients (46%) were men. The most common symptoms were fever (60[87%]), cough (38[55%]), and fatigue (29[42%]). Most patients received antiviral therapy (66 [98.5%] of 67 patients) and antibiotic therapy (66 [98.5%] of 67 patients). As of February 4, 2020, 18 (26.9%) of 67 patients had been discharged, and five patients had died, with a mortality rate of 7.5%. According to the lowest SpO2 during admission, cases were divided into the SpO2≥90% group (n=55) and the SpO2<90% group (n=14). All 5 deaths occurred in the SpO2<90% group. Compared with SpO2≥90% group, patients of the SpO2<90% group were older, and showed more comorbidities and higher plasma levels of IL6, IL10, lactate dehydrogenase, and c reactive protein. Arbidol treatment showed tendency to improve the discharging rate and decrease the mortality rate.
COVID-19 appears to show frequent fever, dry cough, and increase of inflammatory cytokines, and induced a mortality rate of 7.5%. Older patients or those with underlying comorbidities are at higher risk of death.

Hier is ook een mooi overzicht van betrouwbare, peer-reviewed Corona berichtgeving:
https://decorrespondent.n(...)09944-d9fdf3ca#about
https://decorrespondent.n(...)09944-d9fdf3ca#about
Dit is gewoon raar :l


Nieuw artikel:
Viral Invasion and Type I Interferon Response Characterize the Immunophenotypes during COVID-19 Infection
The new coronavirus COVID-19 has spread globally and caused a pneumonia outbreak. Although the whole genome sequences of COVID-19 have been rapidly obtained, pathogenesis of COVID-19 caused severe disease remains elusive. Understanding the immune responses in patients with severe disease may significantly advance the development of effective therapies. Here, using scRNA-seq technology, we profiled the immunophenotypes of four patients’ PBMCs before, during, and after their ICU cares. Our data identified gene expression signatures of viral invasion and type I interferon (IFN-I) responses as the key manifestations characterized the life-threatening stage of COVID-19 infection in human. The association between viral load/IFN-α levels and disease severity in COVID-19 infection marked the key difference in the pathogenesis of this new coronavirus from previous coronavirus such as SARS-CoV infections.
Viral Invasion and Type I Interferon Response Characterize the Immunophenotypes during COVID-19 Infection
The new coronavirus COVID-19 has spread globally and caused a pneumonia outbreak. Although the whole genome sequences of COVID-19 have been rapidly obtained, pathogenesis of COVID-19 caused severe disease remains elusive. Understanding the immune responses in patients with severe disease may significantly advance the development of effective therapies. Here, using scRNA-seq technology, we profiled the immunophenotypes of four patients’ PBMCs before, during, and after their ICU cares. Our data identified gene expression signatures of viral invasion and type I interferon (IFN-I) responses as the key manifestations characterized the life-threatening stage of COVID-19 infection in human. The association between viral load/IFN-α levels and disease severity in COVID-19 infection marked the key difference in the pathogenesis of this new coronavirus from previous coronavirus such as SARS-CoV infections.
Ook een nieuw artikel:
Potentialdual therapeutic approach against SARS-CoV-2/COVID-19 with Nitazoxanide and Hydroxychloroquine
Coronaviruses are ubiquitous in nature and infectsdiverse species with frequent cross-species transmission. There have been multipleevents of animal to human transmission throughout historyincludingSARS,MERS and most recently SARS-CoV-2(COVID-19)that is responsible for the current pandemic. The rapid spread of SARS-CoV-2/COVID-19 has overwhelmed the capabilities of major nations due to the sheer number of patients with severe disease and critically ill patients requiring intensive care. The high molecular and clinical similarity between SARS and SARS-CoV-2 enable us to draw some parallels between them and utilize nearly two decades of existing researchfrom SARS. Herein I describe a Novel synergistictherapeutic approach against SARS-CoV-2/COVID-19 by repurposing Nitazoxanide and Hydroxychloroquineto target viral and host factors for controlling this disease. Both these drugs are readily available, expected to be highly potent andcan be administered at the population level to ensure infected patients do not advance to the point of needing prolonged hospitalization and critical care thereby changing the course of this disease. The proposed treatment regimen would be expected to diminish the severity of illness by reducing viral titersandrescuing the innate-immune system dysregulation brought about by the viral infection that underlies the high mortality in the older/vulnerable populations there by allowing our health-care system a more controlled disease response.
Potentialdual therapeutic approach against SARS-CoV-2/COVID-19 with Nitazoxanide and Hydroxychloroquine
Coronaviruses are ubiquitous in nature and infectsdiverse species with frequent cross-species transmission. There have been multipleevents of animal to human transmission throughout historyincludingSARS,MERS and most recently SARS-CoV-2(COVID-19)that is responsible for the current pandemic. The rapid spread of SARS-CoV-2/COVID-19 has overwhelmed the capabilities of major nations due to the sheer number of patients with severe disease and critically ill patients requiring intensive care. The high molecular and clinical similarity between SARS and SARS-CoV-2 enable us to draw some parallels between them and utilize nearly two decades of existing researchfrom SARS. Herein I describe a Novel synergistictherapeutic approach against SARS-CoV-2/COVID-19 by repurposing Nitazoxanide and Hydroxychloroquineto target viral and host factors for controlling this disease. Both these drugs are readily available, expected to be highly potent andcan be administered at the population level to ensure infected patients do not advance to the point of needing prolonged hospitalization and critical care thereby changing the course of this disease. The proposed treatment regimen would be expected to diminish the severity of illness by reducing viral titersandrescuing the innate-immune system dysregulation brought about by the viral infection that underlies the high mortality in the older/vulnerable populations there by allowing our health-care system a more controlled disease response.
En deze:
https://www.mediterranee-(...)e_final_DOI_IJAA.pdf
Combinatie van Azythromycine en Hydrochloroquine heeft 8 patienten genezen tov 1 patient in de controlegroup.
https://www.mediterranee-(...)e_final_DOI_IJAA.pdf
Combinatie van Azythromycine en Hydrochloroquine heeft 8 patienten genezen tov 1 patient in de controlegroup.
Super deze:
https://www.bddataplan.nl/corona/
https://www.bddataplan.nl/corona/
- edit: adverteren kan middels een mail naar pr@fok.nl -
Toch even hier (Informatie van Artsen voor Longziekten en Tuberculose (NVALT) ), ondanks het een AD.nl artikel is. Voor al die mensen lopen te roepen dat allerlei middelen gebruikt moeten worden.
quote:Longartsen met handen in haar: ‘Aanbevolen medicijnen hebben niet veel effect, maar wel bijwerkingen’
Longartsen zitten met hun handen in het haar omdat er geen effectieve behandeling is voor het coronavirus. In een nieuwe Nederlandse richtlijn die specialisten gisteren met elkaar bespraken, staat dat er nog onvoldoende bewijs is voor de werking van de in de richtlijn genoemde medicijnen. Sommigen richten wellicht zelfs meer schade aan dan dat ze goed doen. ,,In de praktijk zien we in Brabant tot nu toe niet veel effect van die medicijnen, maar hebben patiënten wel last van bijwerkingen.’’
De eerste behandelresultaten stemmen de voorzitter van de Nederlandse Vereniging van Artsen voor Longziekten en Tuberculose (NVALT) Leon van den Toorn treurig. ,,Wat we tot nu toe in de praktijk zien in de regio Brabant is dat de aanbevolen medicijnen niet veel effect lijken te hebben’’, verklaart Van den Toorn. ,,Maar patiënten hebben in ieder geval wel last van bijwerkingen, zoals depressieve klachten, misselijkheid en braken.’’
Hartritmestoornissen
In de databank voor bijwerkingen Lareb staat dat chloroquine naast maagdarmklachten en hoofdpijn bijvoorbeeld ook ernstige hartklachten en hartritmestoornissen kan veroorzaken. ,,Gebruik dit medicijn NIET als u deze hartritmestoornis heeft’’, klinkt het dringende advies.
Volgens de longarts, die zelf werkzaam is in het Rotterdamse Erasmus MC is het middel dat ‘in Nederland verreweg het meest geprobeerd wordt ‘chloroquine’, een medicijn dat ook gebruikt wordt om malaria te voorkomen. ,,Niet alle ziekenhuizen zijn er enthousiast over, maar de in meeste ziekenhuizen wordt het wel gegeven bij de ziekere patiënten.’’ Of er in Nederland mensen gered zijn met dat middel? ,,Zo kun je dat niet zeggen, heel veel weten we er nog niet over’’, erkent de voorman. Bovendien benadrukt hij: ,,Je weet natuurlijk ook niet wat er met die mensen was gebeurd als je het middel níet had toegepast.’’
Reageerbuisjes
Longartsen staan mede door het gebrek aan bewijs voor grote dilemma’s bij de behandeling van coronapatiënten. ,,In lekentaal komt het er simpel gezegd op neer dat de medicijnen in reageerbuisjes zijn onderzocht’’, legt Van den Toorn uit. ,,In het laboratorium zijn er aanwijzingen dat die medicijnen mogelijk iets tegen het virus doen, maar we weten nog niet of dat daadwerkelijk het geval is als je er mensen mee behandelt.’’
De voorzitter van de longartsen pleit voor gedegen onderzoek naar de medicijnen die tot nu toe geprobeerd zijn tegen het nieuwe coronavirus. Hij krijgt bijval van arts-microbioloog Marc Bonten uit het UMC Utrecht: ,,De middelen die er nu zijn moeten getest worden op twee dingen: één, of ze mensen beter maken, en twee, of ze veilig gebruikt kunnen worden. Die middelen moeten op grote schaal bij mensen gebruikt gaan worden, om te zien of ze effect hebben.’’
Testen op mensen
De Rotterdamse longarts Hans in ‘t Veen uit het Franciscus Gasthuis en Vlietland herkent de moeilijkheden. ,,Er zijn drie problemen: De medicatie is niet beschikbaar, de medicatie is vaak toxisch en we weten zelfs niet eens of het helpt.’’ Volgens hem gaat er over die richtlijn ‘zeker veel discussie’ komen. ,,Als het niet bewezen is en heel schadelijk is: moet je de vraag stellen of je de behandelingsadviezen zo nadrukkelijk kan opschrijven?’’ zo nuanceert hij de aanbeveling hardop.
Om te achterhalen of de middelen werken moeten mensen min of meer gaan functioneren als proefkonijn. Bonten: ,,Het zijn helaas echte mensen die je daarvoor nodig hebt, maar je moet die medicijnen onderzoeken. Anders weten we over een half jaar nog steeds niet wat de beste behandeling is.’’
In levensgevaar
De richtlijn beveelt specialisten aan om de omstreden middelen alleen te gebruiken bij patiënten met ‘ernstige klachten’ en als mensen in levensgevaar zijn. Gisteren spraken artsen via een videoconferentie over de richtlijn: ,,De bewijslast voor de middelen die in de richtlijn genoemd worden is helaas flinterdun’’, erkent Van den Toorn. ,,Daarom is er continue overleg, wordt van vele patiënten bijgehouden wat de behandeling is geweest en proberen we daar uiteindelijk wijzer van te worden. Ondertussen wachten we ook op de uitkomsten van studies die nog lopen. Alleen het duurt nog wel even voordat daar de resultaten van binnenkomen: dat gaat niet in een week.’’
Naast chloroquine, is er ook nog een een ander malariamedicijn ‘hydroxychloroquine’, ,,Dat lijkt op chloroquine en wordt in sommige ziekenhuizen ook toegepast’’, weet Van den Toorn. En verder is er de virusremmer ‘remdesivir’. Dit middel werd oorspronkelijk gebruikt tegen de extreem dodelijke ziekte ebola, maar viel af omdat andere middelen beter bleken te werken. In Nederland wordt het volgens Van den Toorn nog bijna niet voorgeschreven, omdat dat middel heel slecht beschikbaar is’.
Strijd zonder wapens
Zo lijken de doktoren een oneerlijke strijd te voeren tegen het nieuwe coronavirus dat in steeds meer landen om zich heen slaat. Of je dat een strijd zonder wapens kunt noemen? Van den Toorn geeft toe: ,,Tot nu toe voeren we oorlog zonder goede wapens, maar we gaan er desondanks vanuit dat we de strijd uiteindelijk gaan winnen. Bovendien knapt het overgrote deel van de patiënten op, óók zonder die medicijnen, dus dat geeft hoop.’’



Hier een NRC artikel over hoe het RIVM de maatregelen zoals bijvoorbeeld sluiten van de scholen ook zeer wetenschappelijk benaderd. Een wiskundige benadering met modellen.
Waarom bierviltjesberekeningen over het virus niet werken
Wiskundige modellen Afstand houden, scholen sluiten, ‘lockdown’: bij het RIVM rekenen hypercomplexe wiskundige modellen alle maatregelen na. NRC sprak er vijf wetenschappers over. „Zonder wiskundige modellen is niet te begrijpen wat je ziet.”
Waarom bierviltjesberekeningen over het virus niet werken
Wiskundige modellen Afstand houden, scholen sluiten, ‘lockdown’: bij het RIVM rekenen hypercomplexe wiskundige modellen alle maatregelen na. NRC sprak er vijf wetenschappers over. „Zonder wiskundige modellen is niet te begrijpen wat je ziet.”
Artikel over Ijsland waar ze de gehele bevolking kunnen gaan testen.
Iceland finds half of positive cases have no disease traits
https://www.bloomberg.com(...)symptom-scmp-reports
en hier een statement van de Ijslandse regering
https://www.government.is(...)in-Iceland-underway/
Iceland finds half of positive cases have no disease traits
https://www.bloomberg.com(...)symptom-scmp-reports
en hier een statement van de Ijslandse regering
https://www.government.is(...)in-Iceland-underway/
quote:• Iceland has tested 9 768 individuals for COVID-19, which translates to 26 762 per million, compared with 6 343 in South Korea and 13 999 in Bahrein
• Iceland has tested a higher proportion of inhabitants than any other country after deCode genetics started offering free screening among the general, non-symptomatic, non-quarantined population
• deCode has published the results of a total of 5 571 tests. Those have yielded 48 positive results (0.86%) indicating that the prevelance of the virus is modest among the general population.
• A total of 473 cases have been identified in Iceland since the first case on February 28th. One person with COVID-19 has died. Twelve individuals with COVID-19 are hospitalized.
https://equalocean.com/he(...)ia-ct-lung-screening
quote:Infervision: Our AI Detects Deadly Coronavirus via CT Lung Screening
The lung cancer detection company has launched a deep learning-based coronavirus detection system in Wuhan.
Infervision (推想科技) described its coronavirus detection model as working through CT lung screening. This means that the new model detects ground-glass opacities (GGO) in the lung that may later be confirmed as one of the complications of the virus.
The firm's model has already been used by Wuhan Tongji Hospital, one of the frontline hospitals that has been fighting with the epidemic in Wuhan. It is set to be deployed in multiple other hospitals in the near future, Infervision said.
“It serves as a surrogate to PCR diagnostic as the lab capacities aren't enough to keep up with the rising number of suspected cases in the afflicted regions," added the company.
Another diagnostics solution support for the rising crisis was launched by Shenzhen-based genomics giant BGI Genomics (300676: SH) on January 28. The company's stocks opened around 10% up as the mainland's stock markets open on January 3, 2020.
“The new coronavirus may cause infections with no symptoms and sicken otherwise healthy people,” postulated the Lancet, showing how hard it is presently for hospitals in Wuhan, which are racing against time to diagnose large numbers of patients.
The new diagnostic solutions possess tremendous importance for the afflicted region, considering the symptoms of the new virus are similar to other fast-spreading diseases like flu, complicating the process and creating excess demand thanks to a large number of concerned patients who need to be assessed. "Symptomatic patients are piling up in the hospital – AI can help triage the patients quickly," said the firm. "Patients have been seen without any noticeable symptoms like fever or cough, but showing large GGOs in the lung,"
The Beijing-based private firm had long been drawing the attention of wealthy venture capitalists, including Qiming Venture Partners and Sequoia China; it has secured around USD 100 million since its inception in January 2016. The team has been adopting deep learning technology broadly in the medical imaging field.
The firm was involved in an early victory in this complex battle: for the first time since the emergence of the new virus in late 2019, the number of new suspected coronavirus cases in China started to drop, over two consecutive days, on December 31 and January 1, 2020 - mostly driven by faster diagnostic solutions. PCR diagnostics had shown that it could play a crucial role.
Wer lesen kann, ist klar im Vorteil.
Op weather.com staat een interactieve kaart waar Amerikanen (en wij  )op county-niveau het aantal gevallen kunnen zien (plaatsnaam invullen dan kun je in/uitzoomen):
)op county-niveau het aantal gevallen kunnen zien (plaatsnaam invullen dan kun je in/uitzoomen):
https://weather.com/coronavirus/
https://weather.com/coronavirus/
Wer lesen kann, ist klar im Vorteil.
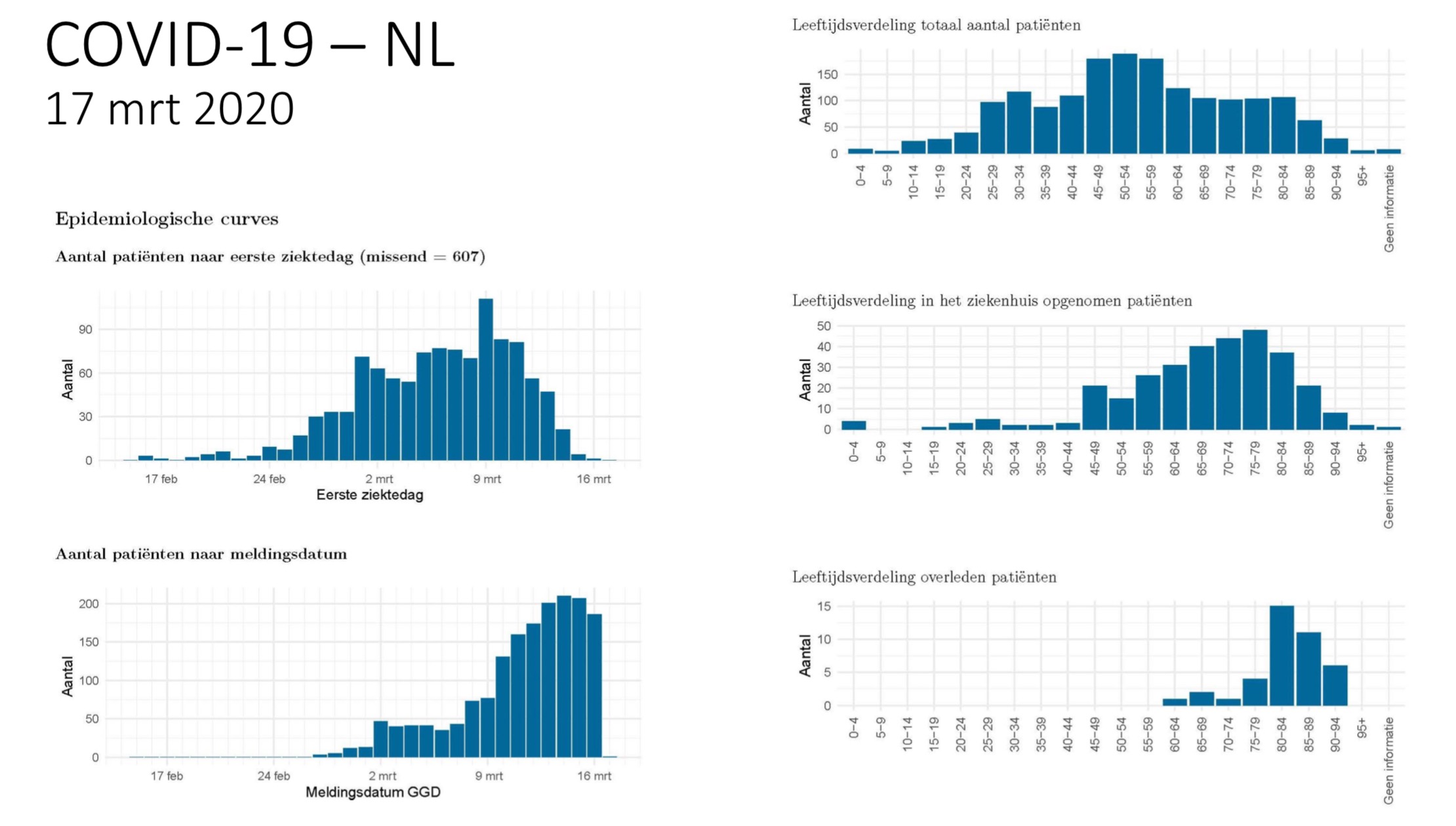
Epidemiologische situatie COVID-19 in Nederland 25 maart 2020
Samenvatting
Tot en met 25 maart 2020 zijn er in Nederland in totaal 6412 COVID-19 patiënten gemeld aan het RIVM Rijksinstituut voor Volksgezondheid en Milieu . De meeste gemelde patiënten vallen in de leeftijdscategorie 55-59 jaar. Tot nu toe zijn van deze gemelde patiënten 1836 opgenomen in het ziekenhuis en 356 overleden.
De meeste overleden patiënten zaten in de leeftijdscategorie 80-84 jaar.
https://www.rivm.nl/documenten/epidemiologische-situatie-covid-19-in-nederland-25-maart-2020
Samenvatting
Tot en met 25 maart 2020 zijn er in Nederland in totaal 6412 COVID-19 patiënten gemeld aan het RIVM Rijksinstituut voor Volksgezondheid en Milieu . De meeste gemelde patiënten vallen in de leeftijdscategorie 55-59 jaar. Tot nu toe zijn van deze gemelde patiënten 1836 opgenomen in het ziekenhuis en 356 overleden.
De meeste overleden patiënten zaten in de leeftijdscategorie 80-84 jaar.
https://www.rivm.nl/documenten/epidemiologische-situatie-covid-19-in-nederland-25-maart-2020
Treatment of COVID-19 with Individualized Immune Boosting Interventions
There are major concerns regarding the current global pandemic of coronavirus disease 2019 (COVID-19) caused by the coronavirus SARS-CoV-2. Whereas most of the infected individuals have no symptoms or only mild symptoms, in a small minority, the infection can lead to pneumonia and death. One major concern regarding the pandemic is the 2.3% average case fatality rate of the COVID-19 patients, with the fatality rate increasing to 8% for patients aged 70 to 79 and 14.8% for those aged 80 and over. Another major concern is the person-to-person transmission of the coronavirus by asymptomatic individuals during the incubation period, making it difficult to limit the spread of the disease. Many steps are underway worldwide to limit the spread of the disease, e.g. cancellation of conferences and large gatherings, closure of schools, curtailment of travel, etc. Considering the magnitude of the adverse impact on the social, cultural, commercial, educational, scientific, health, and other aspects of the society from such steps and the large anticipated casualties with the expected spread of the disease worldwide, it is important to explore methods of reducing the fatality rates of COVID-19 patients. Since the weakness of the immune system is one of the major contributing factors for the occurrence of pneumonia, and inflammation contributes to increased mortality rates of pneumonia patients, interventions that improve the immune response and/or reduce inflammation may reduce the pneumonia incidence and mortality in COVID-19 patients. There are indeed a large number of interventions that improve the immune response and/or reduce inflammation. However, all the interventions would not be applicable or acceptable to everyone and so the interventions would need to be individualized based on individual circumstances and preferences. This approach, known as “Individualized Interventions to Improve the Immune Response”, or the I4R approach needs to be tested in pilot clinical trials for the treatment of COVID-19 patients. If the pilot clinical trials demonstrate that it is effective in reducing the incidence and mortality due to pneumonia, widespread adoption of the I4R approach for treating COVID-19 patients may reduce their morbidity and mortality, reducing the concerns regarding the coronavirus. This may be helpful in reducing the need for the drastic steps that have been taken worldwide, and help in the return of life to normalcy. Therefore, clinical trials of the I4R approach should be conducted on an urgent basis.
There are major concerns regarding the current global pandemic of coronavirus disease 2019 (COVID-19) caused by the coronavirus SARS-CoV-2. Whereas most of the infected individuals have no symptoms or only mild symptoms, in a small minority, the infection can lead to pneumonia and death. One major concern regarding the pandemic is the 2.3% average case fatality rate of the COVID-19 patients, with the fatality rate increasing to 8% for patients aged 70 to 79 and 14.8% for those aged 80 and over. Another major concern is the person-to-person transmission of the coronavirus by asymptomatic individuals during the incubation period, making it difficult to limit the spread of the disease. Many steps are underway worldwide to limit the spread of the disease, e.g. cancellation of conferences and large gatherings, closure of schools, curtailment of travel, etc. Considering the magnitude of the adverse impact on the social, cultural, commercial, educational, scientific, health, and other aspects of the society from such steps and the large anticipated casualties with the expected spread of the disease worldwide, it is important to explore methods of reducing the fatality rates of COVID-19 patients. Since the weakness of the immune system is one of the major contributing factors for the occurrence of pneumonia, and inflammation contributes to increased mortality rates of pneumonia patients, interventions that improve the immune response and/or reduce inflammation may reduce the pneumonia incidence and mortality in COVID-19 patients. There are indeed a large number of interventions that improve the immune response and/or reduce inflammation. However, all the interventions would not be applicable or acceptable to everyone and so the interventions would need to be individualized based on individual circumstances and preferences. This approach, known as “Individualized Interventions to Improve the Immune Response”, or the I4R approach needs to be tested in pilot clinical trials for the treatment of COVID-19 patients. If the pilot clinical trials demonstrate that it is effective in reducing the incidence and mortality due to pneumonia, widespread adoption of the I4R approach for treating COVID-19 patients may reduce their morbidity and mortality, reducing the concerns regarding the coronavirus. This may be helpful in reducing the need for the drastic steps that have been taken worldwide, and help in the return of life to normalcy. Therefore, clinical trials of the I4R approach should be conducted on an urgent basis.
Covid-19 fatality is likely overestimated
The final case fatality rate (CFR) from SARS-CoV-2, the virus that causes covid-19, will likely be lower than those initially reported.1 Previous reviews of H1N1 and SARS show the systematic inflation of early mortality estimates.23 Early estimates of H1N1’s mortality were susceptible to uncertainty about asymptomatic and subclinical infections, heterogeneity in approaches to diagnostic testing, and biases in confounding, selection, detection, reporting, and so on.23 These biases are difficult to overcome early in a pandemic.3
We read Xu and colleagues’ report of 62 cases of covid-19 outside of Wuhan, China, with interest, as no patients died in the study period.5 Compared with a report of the 72 314 cases throughout China, the marked differences in outcomes from Hubei (the province of which Wuhan is the capital) compared with all other provinces are worth a brief discussion.4
The CFR in China (through 11 February) is reported as 2.3%.15 The CFR among the initial Wuhan cohort was reported as 4.3%, with a rate of 2.9% in Hubei province.15 But outside Hubei the CFR has been 0.4%. Deaths occurred only in cases deemed “critical.” Importantly, the CFR from these reports is from infected, syndromic people presenting to healthcare facilities, with higher CFRs among older patients in hospital (8%-14.8% in the Wuhan cohort).
As accessibility and availability of testing for the novel coronavirus increases, the measured CFR will continue to drop, especially as subclinical and mild cases are identified.678 Alternatively, the CFR might not fall as much as in previous epidemics and pandemics, given the prolonged disease course of covid-19 or if mitigation measures or hospital resources prove inadequate.9101112
As with other pandemics, the final CFR for covid-19 will be determined after the pandemic and should not distract from the importance of aggressive, early mitigation to minimise spread of infection.
The final case fatality rate (CFR) from SARS-CoV-2, the virus that causes covid-19, will likely be lower than those initially reported.1 Previous reviews of H1N1 and SARS show the systematic inflation of early mortality estimates.23 Early estimates of H1N1’s mortality were susceptible to uncertainty about asymptomatic and subclinical infections, heterogeneity in approaches to diagnostic testing, and biases in confounding, selection, detection, reporting, and so on.23 These biases are difficult to overcome early in a pandemic.3
We read Xu and colleagues’ report of 62 cases of covid-19 outside of Wuhan, China, with interest, as no patients died in the study period.5 Compared with a report of the 72 314 cases throughout China, the marked differences in outcomes from Hubei (the province of which Wuhan is the capital) compared with all other provinces are worth a brief discussion.4
The CFR in China (through 11 February) is reported as 2.3%.15 The CFR among the initial Wuhan cohort was reported as 4.3%, with a rate of 2.9% in Hubei province.15 But outside Hubei the CFR has been 0.4%. Deaths occurred only in cases deemed “critical.” Importantly, the CFR from these reports is from infected, syndromic people presenting to healthcare facilities, with higher CFRs among older patients in hospital (8%-14.8% in the Wuhan cohort).
As accessibility and availability of testing for the novel coronavirus increases, the measured CFR will continue to drop, especially as subclinical and mild cases are identified.678 Alternatively, the CFR might not fall as much as in previous epidemics and pandemics, given the prolonged disease course of covid-19 or if mitigation measures or hospital resources prove inadequate.9101112
As with other pandemics, the final CFR for covid-19 will be determined after the pandemic and should not distract from the importance of aggressive, early mitigation to minimise spread of infection.






The Impact of Cross-Cultural Differences in Handwashing Patterns on the COVID-19 Outbreak Magnitude
Frequent handwashing with soap for at least 20 seconds at a time is widely advised as one of the preventive measures against COVID-19. Yet, while it is possible to quickly influence individual hygiene behaviorin the short term, in the long run, changing handwashing culture in a particular country as well as globally is a much more difficult task. Considering the relative stability of cross-cultural differencesover time, we explorewhether and to what extent handwashing culture can be used to explain and predict the relative penetration of COVID-19 pandemicinternationally. We find that even though many different factors could have influenced the rapid expansion of the virus, handwashing culture is a very good predictor of the COVID-19 spread magnitude.
Frequent handwashing with soap for at least 20 seconds at a time is widely advised as one of the preventive measures against COVID-19. Yet, while it is possible to quickly influence individual hygiene behaviorin the short term, in the long run, changing handwashing culture in a particular country as well as globally is a much more difficult task. Considering the relative stability of cross-cultural differencesover time, we explorewhether and to what extent handwashing culture can be used to explain and predict the relative penetration of COVID-19 pandemicinternationally. We find that even though many different factors could have influenced the rapid expansion of the virus, handwashing culture is a very good predictor of the COVID-19 spread magnitude.
Covid-19: Data analysis of the Lombardy region and the provinces of Bergamo and Brescia
The data analysis on deaths in the Lombardy Region and of both the provinces of Bergamo and Brescia shows a twofold aspect on the trend of the epidemic: - all the data show a bias linked to the event of March 10th (day for which the Lombardy region data is partial) and the subsequent change in the way in which positive cases and deaths are calculated; - following the containment measures of the Prime Minister's Decree of March 11th, the spread of the epidemic, although still exponential in nature, has a reduced multiplication coefficient. Our analysis concludes that the situation is not yet compatible with a plateau trend and allows us to predict the trend in the number of deaths in the Lombardy region. We therefore conclude that the containment measures put in place by the government on March 11th will allow a reduction in deaths from around 8000 to just over 6500 for March 27th.
The data analysis on deaths in the Lombardy Region and of both the provinces of Bergamo and Brescia shows a twofold aspect on the trend of the epidemic: - all the data show a bias linked to the event of March 10th (day for which the Lombardy region data is partial) and the subsequent change in the way in which positive cases and deaths are calculated; - following the containment measures of the Prime Minister's Decree of March 11th, the spread of the epidemic, although still exponential in nature, has a reduced multiplication coefficient. Our analysis concludes that the situation is not yet compatible with a plateau trend and allows us to predict the trend in the number of deaths in the Lombardy region. We therefore conclude that the containment measures put in place by the government on March 11th will allow a reduction in deaths from around 8000 to just over 6500 for March 27th.
A simplified model for expected development of the SARS-CoV-2 (Corona) spread in Germany and US after social distancing
Widespread opinions and discussion exist regarding the efficiency of social distancing after crucial spread of the SARS-CoV-2 virus during the actual Covid-19 pandemic. While Germany has released a federal law that prohibits any type of direct contact for more than 2 people other countries including the US released curfews.
People are now wondering whether these measures are helpful to stop or hamper the Covid-19 pandemic and to limit the spread of the new corona virus.
A quantitative statement on this question depends on many parameters that are difficult to grasp mathematically and cannot therefore be made conclusively (they include consistent adherence to the measures decided, the estimated number of unreported cases, the possible limitation by test capacities, possible mutations of the virus, etc ...). However, it turns out that a reduction in the actual daily new infection rate (actual daily growth rate of reported cases, in short: infection rate) from the current value of 30-35% in the US to 10% would be extremely effective in stopping the spread of the virus. The severe restrictions in Germany which closed any public events, schools and universities a week ago might already have contributed to a reduction of the growth rate of reported cases below 30%.
Widespread opinions and discussion exist regarding the efficiency of social distancing after crucial spread of the SARS-CoV-2 virus during the actual Covid-19 pandemic. While Germany has released a federal law that prohibits any type of direct contact for more than 2 people other countries including the US released curfews.
People are now wondering whether these measures are helpful to stop or hamper the Covid-19 pandemic and to limit the spread of the new corona virus.
A quantitative statement on this question depends on many parameters that are difficult to grasp mathematically and cannot therefore be made conclusively (they include consistent adherence to the measures decided, the estimated number of unreported cases, the possible limitation by test capacities, possible mutations of the virus, etc ...). However, it turns out that a reduction in the actual daily new infection rate (actual daily growth rate of reported cases, in short: infection rate) from the current value of 30-35% in the US to 10% would be extremely effective in stopping the spread of the virus. The severe restrictions in Germany which closed any public events, schools and universities a week ago might already have contributed to a reduction of the growth rate of reported cases below 30%.
Clinical Characteristics of Fatal and Recovered Cases of Coronavirus Disease 2019 (COVID-19) in Wuhan, China: A Retrospective Study
The 2019 novel coronavirus (2019-nCoV) has caused the outbreak of the acute respiratory disease in Wuhan, Hubei Province of China since December 2019. This study is performed to analyze the clinical characteristics of patients who succumbed to and who recovered from 2019 novel coronavirus disease (COVID-19).Clinical data were collected from two tertiary hospitals in Wuhan. A retrospective investigation was conducted to analyze the clinical characteristics of fatal cases of COVID-19 (death group) and compare them with recovered patients (recovered group). Continuous variables were analyzed using the Mann-Whitney U test. Categorical variables were analyzed by χ test or Fisher's exact tests as appropriate.
The 2019 novel coronavirus (2019-nCoV) has caused the outbreak of the acute respiratory disease in Wuhan, Hubei Province of China since December 2019. This study is performed to analyze the clinical characteristics of patients who succumbed to and who recovered from 2019 novel coronavirus disease (COVID-19).Clinical data were collected from two tertiary hospitals in Wuhan. A retrospective investigation was conducted to analyze the clinical characteristics of fatal cases of COVID-19 (death group) and compare them with recovered patients (recovered group). Continuous variables were analyzed using the Mann-Whitney U test. Categorical variables were analyzed by χ test or Fisher's exact tests as appropriate.
Totaal aantal meldingen per gemeente. De laatste paar dagen worden iets langer getoond.
Totaal aanntal meldingen per 100.000 inwoners. Vooral de gemeente Boekel en aanliggende worden hard getroffen.
De meeste nieuwe meldingen zijn in Amsterdam en Rotterdam de laatste dagen.
@George_of_the_Jungle

Totaal aanntal meldingen per 100.000 inwoners. Vooral de gemeente Boekel en aanliggende worden hard getroffen.

De meeste nieuwe meldingen zijn in Amsterdam en Rotterdam de laatste dagen.

@George_of_the_Jungle

Estimating the number of infections and the impact of non-pharmaceutical interventions on COVID-19 in 11 European countries
Deze is wel interessant qua geschatte deel van de bevolking dat besmet is.

Deze is wel interessant qua geschatte deel van de bevolking dat besmet is.
Ik betwijfel of het model erg goed daarvoor geschikt is...quote:Op dinsdag 31 maart 2020 09:48 schreef Momo het volgende:
Estimating the number of infections and the impact of non-pharmaceutical interventions on COVID-19 in 11 European countries
[ afbeelding ]
Deze is wel interessant qua geschatte deel van de bevolking dat besmet is.
als ik dat onderzoek lees presenteren ze hun model eerder als methode om het effect van maatregelen (niet medicinale, dus vooral 'sociale' regelgeving en beinvloedding vand e gemeenschap ) te kunnen onderzoeken, dus hoe werkzaam bv verschillende methodes als campagne's voor social distancing of lockdowns zijn...
de 'schatting' van het exacte aantal geinfecteerden per bevolking is deel daarvan, waarbij ze bewust niet afgaan op aantal positieve cornoa-tests, aangezien dat naturlijk ook sterk afhangt van het aantal tests dat een bepaald land afneemt en hoe toegankelijk die tests zijn (bv duitsland en zuid-korea hebben veel geinfecteerden, maar testen ook erg pro-actief, waar andere landen een tekort aan tests hebben).
het onderzoek heeft een these dat men een aantal geinfecteerden afmeet aan het aantal sterfgevallen drie weken later, wat mogelijk een ietwat correctere weergave is, aangezien minder afhankelijk is van hoeveel tests men afneemt en direkt gekoppeld een een 'gevolg' (overigens lijken me naast sterfgevallen ook ziekenhuisopnames een goed middel, maar misschien waren die cijfers lastiger verkrijgbaar).
Als je landen qua infectieratio werkelijk onderling wilt vergelijken, moet je een paar aanname's dan doen:
- alle onderzochtte landen zouden dan eenzelfde methode aanhouden om sterfgevallen als een corona-patient te detecteren... probleem hierbij is echter dat hierin al gevalen zijn, specifiek duitsland doet niet aan post-mortem testen, waardor vermoedelijk het sterfcijfer van corona-patienten véél lager is
- de sterftekans is ook gelijk per land, wat ook waarschijnlijk niet klopt, bepaalde landen hebben veel meer medische faciliteiten en mogelijk een betere overlvingskans en ook is er een kans dat onder verschillende herkomstgroepen het virus ook een ietwat andere uitwerking heeft.
Ik denk dat dat onderzoek best een goede en interessante methode is om de werkzaamheid van maatschappelijke maatregelen (non-pharmaceutical interventions) te testen...
maar de mogelijkheid er werkelijk verschillende landen onderling mee te vergelijken erg beperkt is.
Sowieso, die infectieratio per 28 maart is enkel hun 'posterior model estimate' dus een schatting gebaseerd op hun berekeningen (op basis van Bayesian statistieken), die pas over drie weken terug te rekenen is op basis van daadwerkelijke sterfgevallen tegen die tijd.
"Whatever you feel like: Life’s not one color, nor are you my only reader" - Ausonius, Epigrammata 25
Warm weer lijkt niet de besmettingskans te reduceren
Association between ambient temperature and COVID-19 infection in 122 cities from China
The exposure-response curves suggested that the relationship between mean temperature and COVID-19 confirmed cases was approximately linear in the range of less than 3 °C and became flat above 3 °C.
•
When mean temperature (lag0-14) was below 3 °C, each 1 °C rise was associated with a 4.861% (95% CI: 3.209-6.513) increase in the daily number of COVID-19 confirmed cases.
•
There is no evidence supporting that case counts of COVID-19 could decline when the weather becomes warmer when the temperature is above 3 °C.
Association between ambient temperature and COVID-19 infection in 122 cities from China
The exposure-response curves suggested that the relationship between mean temperature and COVID-19 confirmed cases was approximately linear in the range of less than 3 °C and became flat above 3 °C.
•
When mean temperature (lag0-14) was below 3 °C, each 1 °C rise was associated with a 4.861% (95% CI: 3.209-6.513) increase in the daily number of COVID-19 confirmed cases.
•
There is no evidence supporting that case counts of COVID-19 could decline when the weather becomes warmer when the temperature is above 3 °C.
Cross-Country Comparison of Case Fatality Rates of COVID-19/SARS-COV-2
Objectives
Case fatality rates (CFR) and recovery rates are important readouts during epidemics and pandemics. In this article, an international analysis was performed on the ongoing coronavirus disease 2019 (COVID-19) pandemic.
Methods
Data were retrieved from accurate databases according to the user’s guide of data sources for patient registries, CFR and recovery rates were calculated for each country. A comparison of CFR between countries with total cases ≥ 1,000 was observed for 12th and 23rd March.
Results
Italy’s CFR was the highest of all countries studied for both time points (12th March, 6.22% versus 23rd March, 9.26%). The data showed that even though Italy was the only European country reported on 12rd March, Spain and France had the highest CFR of 6.16 and 4.21%, respectively, on 23rd March, which was strikingly higher than the overall CFR of 3.61%.
Conclusion
Obtaining detailed and accurate medical history from COVID-19 patients, and analyzing CFR alongside the recovery rate, may enable the identification of the highest risk areas so that efficient medical care may be provided. This may lead to the development of point-of-care tools to help clinicians in stratifying patients based on possible requirements in the level of care, to increase the probabilities of survival from COVID-19 disease.
Objectives
Case fatality rates (CFR) and recovery rates are important readouts during epidemics and pandemics. In this article, an international analysis was performed on the ongoing coronavirus disease 2019 (COVID-19) pandemic.
Methods
Data were retrieved from accurate databases according to the user’s guide of data sources for patient registries, CFR and recovery rates were calculated for each country. A comparison of CFR between countries with total cases ≥ 1,000 was observed for 12th and 23rd March.
Results
Italy’s CFR was the highest of all countries studied for both time points (12th March, 6.22% versus 23rd March, 9.26%). The data showed that even though Italy was the only European country reported on 12rd March, Spain and France had the highest CFR of 6.16 and 4.21%, respectively, on 23rd March, which was strikingly higher than the overall CFR of 3.61%.
Conclusion
Obtaining detailed and accurate medical history from COVID-19 patients, and analyzing CFR alongside the recovery rate, may enable the identification of the highest risk areas so that efficient medical care may be provided. This may lead to the development of point-of-care tools to help clinicians in stratifying patients based on possible requirements in the level of care, to increase the probabilities of survival from COVID-19 disease.
Ik vind het wel een positief initiatief dat alle journals de COVID-19 research gerelateerde artikels gratis ter beschikking lijken te stellen (dat was in ieder geval zo voor alle wetenschappelijjke artikels die ik tot nu toe bekeken heb).
Fijn dat alle artsen, onderzoekers en andere geinteresseerden alles kunnen raadplegen, ook als zij (of de instelling waarvoor ze werken) geen abonnement op dat journal heeft.
Fijn dat alle artsen, onderzoekers en andere geinteresseerden alles kunnen raadplegen, ook als zij (of de instelling waarvoor ze werken) geen abonnement op dat journal heeft.
A Coadunation of Biological and Mathematical Perspectives on the Pandemic COVID-19: A Review
Coronaviruse disease (COVID-19) outbreak has created an emergency globally, and social distancing and isolation is the only solution to prevent its spread. Several countries have announced fully locked on to tackle this pandemic. The recent COVID-2019 has shaken the globe with incidence cases of more than half-million cases, and a mortality toll of more than twenty thousand to date. The coronavirus family is inclusive of pathogen of both – animal species and humans, encapsulating the isolated severe acute respiratory syndrome coronavirus (SARS-CoV). Researchers round the globe have been dexterously working to decode this lethal virus. Many mathematical frameworks have also been depicted which have helped to understand the dynamics of the COVID-19. Research on coronaviruses continues to explore various aspects of viral replication and pathogenesis to understanding the predilection of these viruses to switch between species, to develop an infection in a new host, and to identify significant reservoirs of coronaviruses will dramatically aid in our potential to prophesize when and where potential epidemics may occur. Many of the non-structural and accessory proteins encoded by the viruses remain unclear and unknown. This systematic review highlights the current situation of the pandemic, virus genomic composition, pathogenesis, symptomatology, diagnosis, and prognosis along with mathematical models of disease transmission and dynamics.
Coronaviruse disease (COVID-19) outbreak has created an emergency globally, and social distancing and isolation is the only solution to prevent its spread. Several countries have announced fully locked on to tackle this pandemic. The recent COVID-2019 has shaken the globe with incidence cases of more than half-million cases, and a mortality toll of more than twenty thousand to date. The coronavirus family is inclusive of pathogen of both – animal species and humans, encapsulating the isolated severe acute respiratory syndrome coronavirus (SARS-CoV). Researchers round the globe have been dexterously working to decode this lethal virus. Many mathematical frameworks have also been depicted which have helped to understand the dynamics of the COVID-19. Research on coronaviruses continues to explore various aspects of viral replication and pathogenesis to understanding the predilection of these viruses to switch between species, to develop an infection in a new host, and to identify significant reservoirs of coronaviruses will dramatically aid in our potential to prophesize when and where potential epidemics may occur. Many of the non-structural and accessory proteins encoded by the viruses remain unclear and unknown. This systematic review highlights the current situation of the pandemic, virus genomic composition, pathogenesis, symptomatology, diagnosis, and prognosis along with mathematical models of disease transmission and dynamics.

Dashboard: Covid-19 in Nederland, informatie: landelijk en regionaal.
[ Bericht 2% gewijzigd door Momo op 07-04-2020 18:18:35 ]
[ Bericht 2% gewijzigd door Momo op 07-04-2020 18:18:35 ]
Waarom Europeanen misschien harder getroffen worden door het virus, nog niet peer reviewed maar wel geschikt voor hier.
ACE2 variants underlie interindividual variability and susceptibility to COVID-19 in Italian population
ACE2 variants underlie interindividual variability and susceptibility to COVID-19 in Italian population
Hoe kan Oudewater in de provincie Utrecht zo hoog scoren? Veel grote veeteeltbedrijven in de buurt soms?
OUDEWATER
Bij de tien Nederlandse gemeenten met de meeste coronapatiënten in het ziekenhuis per 100.000 inwoners staat Oudewater op plaats 6. Het is de enige Utrechtse gemeente in dit lijstje. Ook in gemeenten rond Oudewater, zoals Lopik, Montfoort, Woerden en IJsselstein, zijn relatief meer inwoners in het ziekenhuis opgenomen met corona.
https://www.rtvutrecht.nl(...)ekenhuisopnames.html
OUDEWATER
Bij de tien Nederlandse gemeenten met de meeste coronapatiënten in het ziekenhuis per 100.000 inwoners staat Oudewater op plaats 6. Het is de enige Utrechtse gemeente in dit lijstje. Ook in gemeenten rond Oudewater, zoals Lopik, Montfoort, Woerden en IJsselstein, zijn relatief meer inwoners in het ziekenhuis opgenomen met corona.
https://www.rtvutrecht.nl(...)ekenhuisopnames.html

Kun je dit even in een ander topic posten?quote:
Hoe kan Oudewater in de provincie Utrecht zo hoog scoren? Veel grote veeteeltbedrijven in de buurt soms?
OUDEWATER
Bij de tien Nederlandse gemeenten met de meeste coronapatiënten in het ziekenhuis per 100.000 inwoners staat Oudewater op plaats 6. Het is de enige Utrechtse gemeente in dit lijstje. Ook in gemeenten rond Oudewater, zoals Lopik, Montfoort, Woerden en IJsselstein, zijn relatief meer inwoners in het ziekenhuis opgenomen met corona.
https://www.rtvutrecht.nl(...)ekenhuisopnames.html
Dit gaat over statistieken toch?quote:Op woensdag 8 april 2020 12:51 schreef Momo het volgende:
[..]
Kun je dit even in een ander topic posten?

Lees het topic even door dan kan je constateren of het de juiste post is op de juiste plek.quote:
[b] Op Zaterdag 26 april 2008 22:35 schreef lauwert het volgende:[/b]
[i] Waar zouden we toch zijn zonder onze geliefde D_A O+ [/i]
[i] Waar zouden we toch zijn zonder onze geliefde D_A O+ [/i]
Hier lees je ook tegenstrijdige dingen over. Eerst waren het aziaten die veel ace2 receptoren hadden en bv donkere mensen niet(ny statistieken zie je dat niet in terug, los van alle andere factoren).quote:
Waarom Europeanen misschien harder getroffen worden door het virus, nog niet peer reviewed maar wel geschikt voor hier.
ACE2 variants underlie interindividual variability and susceptibility to COVID-19 in Italian population
Zelfde met rokers vs niet rokers.
Als we er hypothetisch vanuit gaan dat ace2 receptoren inderdaad de toegangspoort zijn en hoe meer je hebt des te zieker je wordt.
(Verklaart waarom kinderen en vrouw minder erg ziek worden)
Dan zijn de vervolgvragen voor mij:
- wat zorgt voor veel ace2 receptoren?
- Hoe verlaag je het aantal ace2 receptoren? (Bv dmv medicijn/levensstijl veranderingen)
- is er iets om de toegang mee te blokkeren zodat het virus de receptor niet binnendringt?
Stel het is echt zo dan kan er een manier gevonden worden zodat het virus niet volop binnendringt. Verbeter ook je immuunsysteem en men wordt niet extreem ziek. Corona gereduceerd tot milde griep.
https://erj.ersjournals.c(...)88-2020.article-info
Mensen met chronische obstructieve longziekte (COPD) en mensen die momenteel roken hebben meer ACE2-eiwitten in de longen, precies de eiwitten waarmee SARS-CoV-2 de cel binnenkomt. Deze twee groepen mensen hebben dus een hogere kans op een ernstige vorm van COVID-19, aldus een paper inEuropean Respiratory Journal.
Mensen met chronische obstructieve longziekte (COPD) en mensen die momenteel roken hebben meer ACE2-eiwitten in de longen, precies de eiwitten waarmee SARS-CoV-2 de cel binnenkomt. Deze twee groepen mensen hebben dus een hogere kans op een ernstige vorm van COVID-19, aldus een paper inEuropean Respiratory Journal.
Average detection rate of SARS-CoV-2 infections is estimated around six percent
Zou heel wat zijn als al ongeveer 600.000 mensen besmet waren in Nederland op 31 maart.

Zou heel wat zijn als al ongeveer 600.000 mensen besmet waren in Nederland op 31 maart.
Zuid-Korea doet experimenten om mensen te genezen van covid-19 met bloedplasma behandeling, het lijkt goed te werken.
Use of Convalescent Plasma Therapy in Two COVID-19 Patients with Acute Respiratory Distress Syndrome in Korea
Coronavirus disease 2019 (COVID-19) caused by severe acute respiratory syndrome coronavirus-2 not yet has established its treatment, but convalescent plasma has been expected to increase survival rates as in the case with other emerging viral infections. We describe two cases of COVID-19 treated with convalescent plasma infusion. Both patients presented severe pneumonia with acute respiratory distress syndrome and showed a favorable outcome after the use of convalescent plasma in addition to systemic corticosteroid. To our knowledge, this is the first report of the use of convalescent plasma therapy for COVID-19 in Korea.
Use of Convalescent Plasma Therapy in Two COVID-19 Patients with Acute Respiratory Distress Syndrome in Korea
Coronavirus disease 2019 (COVID-19) caused by severe acute respiratory syndrome coronavirus-2 not yet has established its treatment, but convalescent plasma has been expected to increase survival rates as in the case with other emerging viral infections. We describe two cases of COVID-19 treated with convalescent plasma infusion. Both patients presented severe pneumonia with acute respiratory distress syndrome and showed a favorable outcome after the use of convalescent plasma in addition to systemic corticosteroid. To our knowledge, this is the first report of the use of convalescent plasma therapy for COVID-19 in Korea.
Een grote kans om eventueel ziek te worden van COVID-19 bij mannen die last hebben van haarverlies
Conversations on COVID: Exploring genetic links to COVID-19 severity
An assistant professor of dermatology at Brown’s medical school is investigating whether the genetic cause of hair loss could help to explain greater severity and more fatalities among male COVID-19 patients.
Conversations on COVID: Exploring genetic links to COVID-19 severity
An assistant professor of dermatology at Brown’s medical school is investigating whether the genetic cause of hair loss could help to explain greater severity and more fatalities among male COVID-19 patients.
COVID-19 And Older Adults: What We Know.
SARS-CoV-2, a novel virus that causes COVID-19 infection, has recently emerged and caused a deadly pandemic. Studies have shown that this virus causes worse outcomes and a higher mortality rate in older adults and those with comorbidities such as hypertension, cardiovascular disease, diabetes, chronic respiratory disease, and chronic kidney disease. A significant percentage of older American adults have these diseases, putting them at a higher risk of infection. Additionally, many adults with hypertension, diabetes, and chronic kidney disease are placed on angiotensin-converting enzyme (ACE) inhibitors and angiotensin II receptor blockers (ARBs). Studies have shown that these medications upregulate the ACE-2 receptor, the very receptor which the SARS-CoV-2 virus uses to enter host cells, which puts older adults at a further increased risk of infection. In this review, we discuss the transmission, symptomatology, mortality, and possible treatments for this infection, as they relate to older adults. This article is protected by copyright. All rights reserved.
SARS-CoV-2, a novel virus that causes COVID-19 infection, has recently emerged and caused a deadly pandemic. Studies have shown that this virus causes worse outcomes and a higher mortality rate in older adults and those with comorbidities such as hypertension, cardiovascular disease, diabetes, chronic respiratory disease, and chronic kidney disease. A significant percentage of older American adults have these diseases, putting them at a higher risk of infection. Additionally, many adults with hypertension, diabetes, and chronic kidney disease are placed on angiotensin-converting enzyme (ACE) inhibitors and angiotensin II receptor blockers (ARBs). Studies have shown that these medications upregulate the ACE-2 receptor, the very receptor which the SARS-CoV-2 virus uses to enter host cells, which puts older adults at a further increased risk of infection. In this review, we discuss the transmission, symptomatology, mortality, and possible treatments for this infection, as they relate to older adults. This article is protected by copyright. All rights reserved.
Coronavirus COV-19/SARS-CoV-2 affects women less than men: clinical response to viral infection.
CoV-19/SARS-CoV-2 is a highly pathogenic virus that causes coronavirus-19 disease (COVID-19) an acute respiratory distress syndrome which provokes serious problems for global health. Studies suggest that there are many differences between men and women in the immune response to CoV-19 infection and inflammatory diseases. Women, compared to men, are less susceptible to viral infections based on a different innate immunity, steroid hormones and factors related to sex chromosomes. The presence of two X chromosomes in women emphasize the immune system even if one is inactive. The immune regulatory genes encoded by X chromosome in female gender causes lower viral load levels, and less inflammation than in man, while CD4+ T cells are higher with better immune response. In addition, women generally produce higher levels of antibodies which remain in the circulation longer. The levels of activation of the immune cells are higher in women than in men, and it is correlated with the trigger of TLR7 and the production of IFN. TLR7 is higher in women than in men and its biallelic expression leads to higher immune responses and increases the resistance to viral infections. TLR7 is expressed in innate immune cells which recognizes single strand RNA virus by promoting the production of antibodies against the virus and the generation of pro-inflammatory cytokines including IL-6 and IL-1 family members. Moreover, in women the production of inflammatory IL-6 after viral infection is lower than in males and is often correlated with a better longevity. In addition, on the X chromosome there are loci that code for the genes involved in the regulation of immune cells such as FOXP3, and transcription factor for Treg involved in virus pathogenesis. The X chromosome influences the immune system by acting on many other proteins, including TLR8, CD40L and CXCR3 which can be over-expressed in women, and influence the response to viral infections and vaccinations. However, the biallelic expression of the X-linked genes can promote harmful autoimmune and inflammatory responses. Cardiovascular diseases are more frequent in males and subjects without cardiovascular dysfunctions infected by CoV-19 have a better prognosis. ACE2 is a receptor for CoV-19 and protects lung damage. CoV-19 infection and the virus's Spike protein inhibit the expression of ACE2, abolishing its protective function. Inhibitors of the angiotensin converting enzyme (ACEI) are used to stem the devastating effects of CoV-19, to increase the number of CD3 and CD8 T cells and to reduce the viral load and IL-6 levels that control CoV-19 replication via NF-B, but these effects are still under study. It is hoped that certain drugs, such as CoV-19 receptor blockers, anti-inflammatories (against rheumatic diseases), monoclonal antibodies, anti-IL-1 and anti-IL-6, the remdesevir drug (analogue adenosine, effective against ebola), hydroxychloroquine (for the treatment of malaria) and vaccines, will open up new strategies and new therapeutic ways to combat this terrible virus.
CoV-19/SARS-CoV-2 is a highly pathogenic virus that causes coronavirus-19 disease (COVID-19) an acute respiratory distress syndrome which provokes serious problems for global health. Studies suggest that there are many differences between men and women in the immune response to CoV-19 infection and inflammatory diseases. Women, compared to men, are less susceptible to viral infections based on a different innate immunity, steroid hormones and factors related to sex chromosomes. The presence of two X chromosomes in women emphasize the immune system even if one is inactive. The immune regulatory genes encoded by X chromosome in female gender causes lower viral load levels, and less inflammation than in man, while CD4+ T cells are higher with better immune response. In addition, women generally produce higher levels of antibodies which remain in the circulation longer. The levels of activation of the immune cells are higher in women than in men, and it is correlated with the trigger of TLR7 and the production of IFN. TLR7 is higher in women than in men and its biallelic expression leads to higher immune responses and increases the resistance to viral infections. TLR7 is expressed in innate immune cells which recognizes single strand RNA virus by promoting the production of antibodies against the virus and the generation of pro-inflammatory cytokines including IL-6 and IL-1 family members. Moreover, in women the production of inflammatory IL-6 after viral infection is lower than in males and is often correlated with a better longevity. In addition, on the X chromosome there are loci that code for the genes involved in the regulation of immune cells such as FOXP3, and transcription factor for Treg involved in virus pathogenesis. The X chromosome influences the immune system by acting on many other proteins, including TLR8, CD40L and CXCR3 which can be over-expressed in women, and influence the response to viral infections and vaccinations. However, the biallelic expression of the X-linked genes can promote harmful autoimmune and inflammatory responses. Cardiovascular diseases are more frequent in males and subjects without cardiovascular dysfunctions infected by CoV-19 have a better prognosis. ACE2 is a receptor for CoV-19 and protects lung damage. CoV-19 infection and the virus's Spike protein inhibit the expression of ACE2, abolishing its protective function. Inhibitors of the angiotensin converting enzyme (ACEI) are used to stem the devastating effects of CoV-19, to increase the number of CD3 and CD8 T cells and to reduce the viral load and IL-6 levels that control CoV-19 replication via NF-B, but these effects are still under study. It is hoped that certain drugs, such as CoV-19 receptor blockers, anti-inflammatories (against rheumatic diseases), monoclonal antibodies, anti-IL-1 and anti-IL-6, the remdesevir drug (analogue adenosine, effective against ebola), hydroxychloroquine (for the treatment of malaria) and vaccines, will open up new strategies and new therapeutic ways to combat this terrible virus.
Radiographic and Clinical Features of Children with 2019 Novel Coronavirus (COVID-19) Pneumonia.
OBJECTIVE:
The purpose of this study was to investigate chest computed tomography (CT) findings in children with coronavirus disease-19 (COVID-19) pneumonia in our hospital.
METHODS:
This study included 22 pediatric patients with confirmed COVID-19 from January to March 2020. The chest CT images and clinical data were reviewed.
RESULTS:
The most prevalent presenting symptoms were fever (64%) and cough (59%), and a mildly elevated mean (SD) C-reactive protein (CRP) level of 11.22(11.06) and erythrocyte sedimentation rate of 18.8 (15.17) were detected. The major CT abnormalities observed were mixed ground-glass opacity and consolidation lesions (36%), consolidations (32%), and ground-glass opacities (14%). Peripheral distribution (45%) of lung lesions was predominant. Most of the lesions were multilobar (68%), with an average of three lung segments involved.
CONCLUSION:
Children with COVID-19 had relatively milder symptoms and less severe lung inflammation than adults. Chest CT plays an important role in the management of children with COVID-19 pneumonia.
OBJECTIVE:
The purpose of this study was to investigate chest computed tomography (CT) findings in children with coronavirus disease-19 (COVID-19) pneumonia in our hospital.
METHODS:
This study included 22 pediatric patients with confirmed COVID-19 from January to March 2020. The chest CT images and clinical data were reviewed.
RESULTS:
The most prevalent presenting symptoms were fever (64%) and cough (59%), and a mildly elevated mean (SD) C-reactive protein (CRP) level of 11.22(11.06) and erythrocyte sedimentation rate of 18.8 (15.17) were detected. The major CT abnormalities observed were mixed ground-glass opacity and consolidation lesions (36%), consolidations (32%), and ground-glass opacities (14%). Peripheral distribution (45%) of lung lesions was predominant. Most of the lesions were multilobar (68%), with an average of three lung segments involved.
CONCLUSION:
Children with COVID-19 had relatively milder symptoms and less severe lung inflammation than adults. Chest CT plays an important role in the management of children with COVID-19 pneumonia.
Temporal dynamics in viral shedding and transmissibility of COVID-19
Abstract
We report temporal patterns of viral shedding in 94 patients with laboratory-confirmed COVID-19 and modeled COVID-19 infectiousness profiles from a separate sample of 77 infector–infectee transmission pairs. We observed the highest viral load in throat swabs at the time of symptom onset, and inferred that infectiousness peaked on or before symptom onset. We estimated that 44% (95% confidence interval, 25–69%) of secondary cases were infected during the index cases’ presymptomatic stage, in settings with substantial household clustering, active case finding and quarantine outside the home. Disease control measures should be adjusted to account for probable substantial presymptomatic transmission.
Abstract
We report temporal patterns of viral shedding in 94 patients with laboratory-confirmed COVID-19 and modeled COVID-19 infectiousness profiles from a separate sample of 77 infector–infectee transmission pairs. We observed the highest viral load in throat swabs at the time of symptom onset, and inferred that infectiousness peaked on or before symptom onset. We estimated that 44% (95% confidence interval, 25–69%) of secondary cases were infected during the index cases’ presymptomatic stage, in settings with substantial household clustering, active case finding and quarantine outside the home. Disease control measures should be adjusted to account for probable substantial presymptomatic transmission.

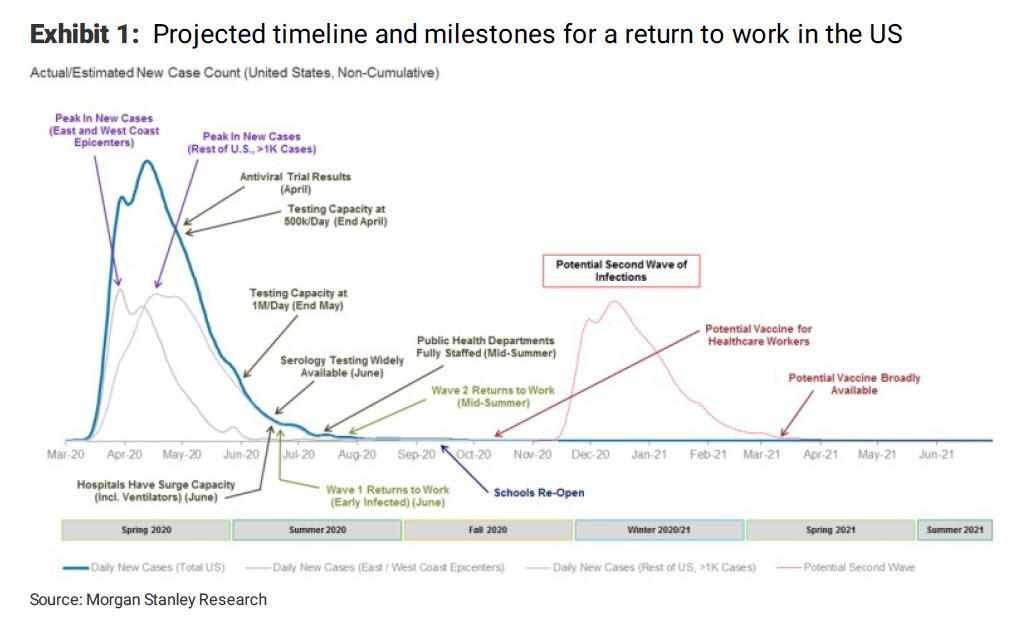

Technische briefings van vandaag in de tweede kamer.
PowerPoint presentatie dhr. Van Dissel - RIVM - Update coronavirus
PowerPoint presentatie mevr. Van Diemen-Steenvoorde - Inspecteur-generaal Inspectie Gezondheidszorg en Jeugd - Update coronavirus
PowerPoint Presentatie dhr. De Gouw - directeur publieke gezondheid GGD en GHOR - Update coronavirus
presentatie mevr. Nieuwenhuizen - voorzitter-bestuurder Verenso - Update coronavirus

PowerPoint presentatie dhr. Van Dissel - RIVM - Update coronavirus
PowerPoint presentatie mevr. Van Diemen-Steenvoorde - Inspecteur-generaal Inspectie Gezondheidszorg en Jeugd - Update coronavirus
PowerPoint Presentatie dhr. De Gouw - directeur publieke gezondheid GGD en GHOR - Update coronavirus
presentatie mevr. Nieuwenhuizen - voorzitter-bestuurder Verenso - Update coronavirus
Technische briefing 8 april
PowerPoint presentatie dhr. Gommers - Nederlandse Vereniging voor Intensive Care - Update coronavirus
PowerPoint presentatie dhr. Van Dissel - RIVM - Update coronavirus
1 april
presentatie Nederlandse Vereniging voor Intensive Care update coronavirus
presentatie RIVM update coronavirus
25 maart
presentatie RIVM Update coronavirus
18 maart
presentatie RIVM over de ontwikkelingen rondom het coronavirus
PowerPoint presentatie dhr. Gommers - Nederlandse Vereniging voor Intensive Care - Update coronavirus
PowerPoint presentatie dhr. Van Dissel - RIVM - Update coronavirus
1 april
presentatie Nederlandse Vereniging voor Intensive Care update coronavirus
presentatie RIVM update coronavirus
25 maart
presentatie RIVM Update coronavirus
18 maart
presentatie RIVM over de ontwikkelingen rondom het coronavirus
Powerpoint presentatie Jaap van Dissel technische briefing 22 april
[ Bericht 28% gewijzigd door Momo op 22-04-2020 14:41:40 ]
[ Bericht 28% gewijzigd door Momo op 22-04-2020 14:41:40 ]
Presenting Characteristics, Comorbidities, and Outcomes Among 5700 Patients Hospitalized With COVID-19 in the New York City Area
Abstract
Importance There is limited information describing the presenting characteristics and outcomes of US patients requiring hospitalization for coronavirus disease 2019 (COVID-19).
Objective To describe the clinical characteristics and outcomes of patients with COVID-19 hospitalized in a US health care system.
Design, Setting, and Participants Case series of patients with COVID-19 admitted to 12 hospitals in New York City, Long Island, and Westchester County, New York, within the Northwell Health system. The study included all sequentially hospitalized patients between March 1, 2020, and April 4, 2020, inclusive of these dates.
Exposures Confirmed severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection by positive result on polymerase chain reaction testing of a nasopharyngeal sample among patients requiring admission.
Abstract
Importance There is limited information describing the presenting characteristics and outcomes of US patients requiring hospitalization for coronavirus disease 2019 (COVID-19).
Objective To describe the clinical characteristics and outcomes of patients with COVID-19 hospitalized in a US health care system.
Design, Setting, and Participants Case series of patients with COVID-19 admitted to 12 hospitals in New York City, Long Island, and Westchester County, New York, within the Northwell Health system. The study included all sequentially hospitalized patients between March 1, 2020, and April 4, 2020, inclusive of these dates.
Exposures Confirmed severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection by positive result on polymerase chain reaction testing of a nasopharyngeal sample among patients requiring admission.
A spatio-temporal analysis for exploring the effect of temperature on COVID-19 early evolution in Spain
Highlights
•
No evidence of a relationship between COVID-19 cases and temperature was found.
•
Results should not be extrapolated to other temperature ranges.
•
These results should be interpreted carefully due to data uncertainty and confounders.
•
It is important to account for non-meteorological, spatial and temporal effects.
Highlights
•
No evidence of a relationship between COVID-19 cases and temperature was found.
•
Results should not be extrapolated to other temperature ranges.
•
These results should be interpreted carefully due to data uncertainty and confounders.
•
It is important to account for non-meteorological, spatial and temporal effects.
Ik plaats dit even hier; als het verkeerd staat hoor ik het wel.
Studie van de Cambridge University over de economische gevolgen van het Coronavirus, de lockdown en van social distancing.
Economic damage could be worse without lockdown and social distancing – study
Economic damage could be worse without lockdown and social distancing – study
"There is much debate over the economic costs of our lockdown lives: whether the price of disease mitigation is worth the risk of an enduring financial crisis.
New research from the University of Cambridge suggests that there is no absolute trade-off between the economy and human health – and that the economic price of inaction could be twice as high as that of a “structured lockdown”.
A Cambridge economist, together with researchers at the US Federal Reserve Board, has combined macroeconomics with aspects of epidemiology to develop a model for the economic consequences of social distancing.
The study uses US economic and population data, but the researchers say their findings have implications for most developed economies.
It divides the working population into “core workers” – those in healthcare as well as food and transportation, sanitation and energy supply, among others – and then everyone else, and models the spread of the virus if no action is taken.
“Without public health restrictions, the random spread of the disease will inevitably hit sectors and industries that are essential for the economy to run,” said co-author Prof Giancarlo Corsetti, from Cambridge’s Faculty of Economics.
“Labour shortfalls among core workers in particular strip more value from the economy. As essential team members within this core sector drop out of the workforce, it impairs production far more than losing those in other areas of the economy.”
By separating the core and non-core workers, the study suggests that the economy would shrink by 30% or more without lockdown and social distancing. “By ignoring this division in the workforce, we may badly underestimate the true depth of economic damage,” Corsetti said.
Read the full story"
SOCIAL DISTANCING AND SUPPLY DISRUPTIONS IN A PANDEMIC
(Cambridge University, Faculty of Economics / Institute for New Economic Thinking)
Abstract
"Drastic public health measures such as social distancing or lockdowns can reduce the loss of human life by keeping the number of infected individuals from exceeding the capacity of the health care system but are often criticized because of the social and the economic cost they entail.
We question this view by combining an epidemiological model, calibrated to capture the spread of the COVID-19 virus, with a multisector model, designed to capture key characteristics of the U.S. Input Output Tables. Our two-sector model features a core sector that produces intermediate inputs not easily replaced by inputs from the other sector, subject to minimum-scale requirements.
We show that, by affecting workers in this core sector, the high peak of an infection not mitigated by social distancing may cause very large upfront economic costs in terms of output, consumption and investment.
Social distancing measures can reduce these costs, especially if skewed towards non-core industries and occupations with tasks that can be performed from home, helping to smooth the surge in infections among workers in the core sector."
Studie van de Cambridge University over de economische gevolgen van het Coronavirus, de lockdown en van social distancing.
Economic damage could be worse without lockdown and social distancing – study
Economic damage could be worse without lockdown and social distancing – study
"There is much debate over the economic costs of our lockdown lives: whether the price of disease mitigation is worth the risk of an enduring financial crisis.
New research from the University of Cambridge suggests that there is no absolute trade-off between the economy and human health – and that the economic price of inaction could be twice as high as that of a “structured lockdown”.
A Cambridge economist, together with researchers at the US Federal Reserve Board, has combined macroeconomics with aspects of epidemiology to develop a model for the economic consequences of social distancing.
The study uses US economic and population data, but the researchers say their findings have implications for most developed economies.
It divides the working population into “core workers” – those in healthcare as well as food and transportation, sanitation and energy supply, among others – and then everyone else, and models the spread of the virus if no action is taken.
“Without public health restrictions, the random spread of the disease will inevitably hit sectors and industries that are essential for the economy to run,” said co-author Prof Giancarlo Corsetti, from Cambridge’s Faculty of Economics.
“Labour shortfalls among core workers in particular strip more value from the economy. As essential team members within this core sector drop out of the workforce, it impairs production far more than losing those in other areas of the economy.”
By separating the core and non-core workers, the study suggests that the economy would shrink by 30% or more without lockdown and social distancing. “By ignoring this division in the workforce, we may badly underestimate the true depth of economic damage,” Corsetti said.
Read the full story"
SOCIAL DISTANCING AND SUPPLY DISRUPTIONS IN A PANDEMIC
(Cambridge University, Faculty of Economics / Institute for New Economic Thinking)
Abstract
"Drastic public health measures such as social distancing or lockdowns can reduce the loss of human life by keeping the number of infected individuals from exceeding the capacity of the health care system but are often criticized because of the social and the economic cost they entail.
We question this view by combining an epidemiological model, calibrated to capture the spread of the COVID-19 virus, with a multisector model, designed to capture key characteristics of the U.S. Input Output Tables. Our two-sector model features a core sector that produces intermediate inputs not easily replaced by inputs from the other sector, subject to minimum-scale requirements.
We show that, by affecting workers in this core sector, the high peak of an infection not mitigated by social distancing may cause very large upfront economic costs in terms of output, consumption and investment.
Social distancing measures can reduce these costs, especially if skewed towards non-core industries and occupations with tasks that can be performed from home, helping to smooth the surge in infections among workers in the core sector."
"The man who never alters his opinion is like standing water, and breeds reptiles of the mind." - William Blake, The Marriage of Heaven and Hell.
Features of 16,749 hospitalised UK patients with COVID-19 using the ISARIC WHO Clinical Characterisation Protocol
Abstract
Objective: To characterize the clinical features of patients with severe COVID-19 in the UK. Design: Prospective observational cohort study with rapid data gathering and near real-time analysis, using a pre-approved questionnaire adopted by the WHO. Setting: 166 UK hospitals between 6th February and 18th April 2020. Participants: 16,749 people with COVID-19. Interventions: No interventions were performed, but with consent samples were taken for research purposes. Many participants were co-enrolled in other interventional studies and clinical trials. Results: The median age was 72 years [IQR 57, 82; range 0, 104], the median duration of symptoms before admission was 4 days [IQR 1,8] and the median duration of hospital stay was 7 days [IQR 4,12]. The commonest comorbidities were chronic cardiac disease (29%), uncomplicated diabetes (19%), non-asthmatic chronic pulmonary disease (19%) and asthma (14%); 47% had no documented reported comorbidity. Increased age and comorbidities including obesity were associated with a higher probability of mortality. Distinct clusters of symptoms were found: 1. respiratory (cough, sputum, sore throat, runny nose, ear pain, wheeze, and chest pain); 2. systemic (myalgia, joint pain and fatigue); 3. enteric (abdominal pain, vomiting and diarrhoea). Overall, 49% of patients were discharged alive, 33% have died and 17% continued to receive care at date of reporting. 17% required admission to High Dependency or Intensive Care Units; of these, 31% were discharged alive, 45% died and 24% continued to receive care at the reporting date. Of those receiving mechanical ventilation, 20% were discharged alive, 53% died and 27% remained in hospital. Conclusions: We present the largest detailed description of COVID-19 in Europe, demonstrating the importance of pandemic preparedness and the need to maintain readiness to launch research studies in response to outbreaks. Trial documentation: Available at https://isaric4c.net/protocols . Ethical approval in England and Wales (13/SC/0149), and Scotland (20/SS/0028). ISRCTN (pending).
Abstract
Objective: To characterize the clinical features of patients with severe COVID-19 in the UK. Design: Prospective observational cohort study with rapid data gathering and near real-time analysis, using a pre-approved questionnaire adopted by the WHO. Setting: 166 UK hospitals between 6th February and 18th April 2020. Participants: 16,749 people with COVID-19. Interventions: No interventions were performed, but with consent samples were taken for research purposes. Many participants were co-enrolled in other interventional studies and clinical trials. Results: The median age was 72 years [IQR 57, 82; range 0, 104], the median duration of symptoms before admission was 4 days [IQR 1,8] and the median duration of hospital stay was 7 days [IQR 4,12]. The commonest comorbidities were chronic cardiac disease (29%), uncomplicated diabetes (19%), non-asthmatic chronic pulmonary disease (19%) and asthma (14%); 47% had no documented reported comorbidity. Increased age and comorbidities including obesity were associated with a higher probability of mortality. Distinct clusters of symptoms were found: 1. respiratory (cough, sputum, sore throat, runny nose, ear pain, wheeze, and chest pain); 2. systemic (myalgia, joint pain and fatigue); 3. enteric (abdominal pain, vomiting and diarrhoea). Overall, 49% of patients were discharged alive, 33% have died and 17% continued to receive care at date of reporting. 17% required admission to High Dependency or Intensive Care Units; of these, 31% were discharged alive, 45% died and 24% continued to receive care at the reporting date. Of those receiving mechanical ventilation, 20% were discharged alive, 53% died and 27% remained in hospital. Conclusions: We present the largest detailed description of COVID-19 in Europe, demonstrating the importance of pandemic preparedness and the need to maintain readiness to launch research studies in response to outbreaks. Trial documentation: Available at https://isaric4c.net/protocols . Ethical approval in England and Wales (13/SC/0149), and Scotland (20/SS/0028). ISRCTN (pending).
Incidence of COVID-19 and Connections with Air Pollution Exposure : Evidence from the Netherlands
Abstract
The fast spread of severe acute respiratory syndrome coronavirus 2 has resulted in the emergence of several hot-spots around the world. Several of these are located in areas associated with high levels of air pollution. This study investigates the relationship between exposure to particulate matter and COVID-19 incidence in 355 municipalities in the Netherlands. The results show that atmospheric particulate matter with diameter less than 2.5 is a highly significant predictor of the number of confirmed COVID-19 cases and related hospital admissions. The estimates suggest that expected COVID-19 cases increase by nearly 100 percent when pollution concentrations increase by 20 percent. The association between air pollution and case incidence is robust in the presence of data on health-related preconditions, proxies for symptom severity, and demographic control variables. The results are obtained with ground-measurements and satellite-derived measures of atmospheric particulate matter as well as COVID-19 data from alternative dates. The findings call for further investigation into the association between air pollution and SARS-CoV-2 infection risk. If particulate matter plays a significant role in COVID-19 incidence, it has strong implications for the mitigation strategies required to prevent spreading.
Abstract
The fast spread of severe acute respiratory syndrome coronavirus 2 has resulted in the emergence of several hot-spots around the world. Several of these are located in areas associated with high levels of air pollution. This study investigates the relationship between exposure to particulate matter and COVID-19 incidence in 355 municipalities in the Netherlands. The results show that atmospheric particulate matter with diameter less than 2.5 is a highly significant predictor of the number of confirmed COVID-19 cases and related hospital admissions. The estimates suggest that expected COVID-19 cases increase by nearly 100 percent when pollution concentrations increase by 20 percent. The association between air pollution and case incidence is robust in the presence of data on health-related preconditions, proxies for symptom severity, and demographic control variables. The results are obtained with ground-measurements and satellite-derived measures of atmospheric particulate matter as well as COVID-19 data from alternative dates. The findings call for further investigation into the association between air pollution and SARS-CoV-2 infection risk. If particulate matter plays a significant role in COVID-19 incidence, it has strong implications for the mitigation strategies required to prevent spreading.
Modeling COVID-19 Growing Trends to Reveal the Differences in the Effectiveness of Non-Pharmaceutical Interventions among Countries in the World
Abstract
Objective: We hypothesize that COVID-19 case growth data reveals the efficacy of NPIs. In this study, we conduct a secondary analysis of COVID-19 case growth data to compare the differences in the effectiveness of NPIs among 16 representative countries in the world. Methods: This study leverages publicly available data to learn patterns of dynamic changes in the reproduction rate for sixteen countries covering Asia, Europe, North America, South America, Australia, and Africa. Furthermore, we model the relationships between the cumulative number of cases and the dynamic reproduction rate to characterize the effectiveness of the NPIs. We learn four levels of NPIs according to their effects in the control of COVID-19 growth and categorize the 16 countries into the corresponding groups. Results: The dynamic changes of the reproduction rate are learned via linear regression models for all of the studied countries, with the average adjusted R-squared at 0.96 and the 95% confidence interval as [0.94 0.98]. China, South Korea, Argentina, and Australia are at the first level of NPIs, which are the most effective. Japan and Egypt are at the second level of NPIs, and Italy, Germany, France, Netherlands, and Spain, are at the third level. The US and UK have the most inefficient NPIs, and they are at the fourth level of NPIs. Conclusions: COVID-19 case growth data provides evidence to demonstrate the effectiveness of the NPIs. Understanding the differences in the efficacy of the NPIs among countries in the world can give guidance for emergent public health events.
Abstract
Objective: We hypothesize that COVID-19 case growth data reveals the efficacy of NPIs. In this study, we conduct a secondary analysis of COVID-19 case growth data to compare the differences in the effectiveness of NPIs among 16 representative countries in the world. Methods: This study leverages publicly available data to learn patterns of dynamic changes in the reproduction rate for sixteen countries covering Asia, Europe, North America, South America, Australia, and Africa. Furthermore, we model the relationships between the cumulative number of cases and the dynamic reproduction rate to characterize the effectiveness of the NPIs. We learn four levels of NPIs according to their effects in the control of COVID-19 growth and categorize the 16 countries into the corresponding groups. Results: The dynamic changes of the reproduction rate are learned via linear regression models for all of the studied countries, with the average adjusted R-squared at 0.96 and the 95% confidence interval as [0.94 0.98]. China, South Korea, Argentina, and Australia are at the first level of NPIs, which are the most effective. Japan and Egypt are at the second level of NPIs, and Italy, Germany, France, Netherlands, and Spain, are at the third level. The US and UK have the most inefficient NPIs, and they are at the fourth level of NPIs. Conclusions: COVID-19 case growth data provides evidence to demonstrate the effectiveness of the NPIs. Understanding the differences in the efficacy of the NPIs among countries in the world can give guidance for emergent public health events.

Incidence of thrombotic complications in critically ill ICU patients with COVID-19
Abstract
Introduction
COVID-19 may predispose to both venous and arterial thromboembolism due to excessive inflammation, hypoxia, immobilisation and diffuse intravascular coagulation. Reports on the incidence of thrombotic complications are however not available.
Methods
We evaluated the incidence of the composite outcome of symptomatic acute pulmonary embolism (PE), deep-vein thrombosis, ischemic stroke, myocardial infarction or systemic arterial embolism in all COVID-19 patients admitted to the ICU of 2 Dutch university hospitals and 1 Dutch teaching hospital.
Results
We studied 184 ICU patients with proven COVID-19 pneumonia of whom 23 died (13%), 22 were discharged alive (12%) and 139 (76%) were still on the ICU on April 5th 2020. All patients received at least standard doses thromboprophylaxis. The cumulative incidence of the composite outcome was 31% (95%CI 20-41), of which CTPA and/or ultrasonography confirmed VTE in 27% (95%CI 17-37%) and arterial thrombotic events in 3.7% (95%CI 0-8.2%). PE was the most frequent thrombotic complication (n = 25, 81%). Age (adjusted hazard ratio (aHR) 1.05/per year, 95%CI 1.004-1.01) and coagulopathy, defined as spontaneous prolongation of the prothrombin time > 3 s or activated partial thromboplastin time > 5 s (aHR 4.1, 95%CI 1.9-9.1), were independent predictors of thrombotic complications.
Conclusion
The 31% incidence of thrombotic complications in ICU patients with COVID-19 infections is remarkably high. Our findings reinforce the recommendation to strictly apply pharmacological thrombosis prophylaxis in all COVID-19 patients admitted to the ICU, and are strongly suggestive of increasing the prophylaxis towards high-prophylactic doses, even in the absence of randomized evidence.
Abstract
Introduction
COVID-19 may predispose to both venous and arterial thromboembolism due to excessive inflammation, hypoxia, immobilisation and diffuse intravascular coagulation. Reports on the incidence of thrombotic complications are however not available.
Methods
We evaluated the incidence of the composite outcome of symptomatic acute pulmonary embolism (PE), deep-vein thrombosis, ischemic stroke, myocardial infarction or systemic arterial embolism in all COVID-19 patients admitted to the ICU of 2 Dutch university hospitals and 1 Dutch teaching hospital.
Results
We studied 184 ICU patients with proven COVID-19 pneumonia of whom 23 died (13%), 22 were discharged alive (12%) and 139 (76%) were still on the ICU on April 5th 2020. All patients received at least standard doses thromboprophylaxis. The cumulative incidence of the composite outcome was 31% (95%CI 20-41), of which CTPA and/or ultrasonography confirmed VTE in 27% (95%CI 17-37%) and arterial thrombotic events in 3.7% (95%CI 0-8.2%). PE was the most frequent thrombotic complication (n = 25, 81%). Age (adjusted hazard ratio (aHR) 1.05/per year, 95%CI 1.004-1.01) and coagulopathy, defined as spontaneous prolongation of the prothrombin time > 3 s or activated partial thromboplastin time > 5 s (aHR 4.1, 95%CI 1.9-9.1), were independent predictors of thrombotic complications.
Conclusion
The 31% incidence of thrombotic complications in ICU patients with COVID-19 infections is remarkably high. Our findings reinforce the recommendation to strictly apply pharmacological thrombosis prophylaxis in all COVID-19 patients admitted to the ICU, and are strongly suggestive of increasing the prophylaxis towards high-prophylactic doses, even in the absence of randomized evidence.
Pandemics, tourism and global change: a rapid assessment of COVID-19
Abstract
The novel coronavirus (COVID-19) is challenging the world. With no vaccine and limited medical capacity to treat the disease, nonpharmaceutical interventions (NPI) are the main strategy to contain the pandemic. Unprecedented global travel restrictions and stay-at-home orders are causing the most severe disruption of the global economy since World War II. With international travel bans affecting over 90% of the world population and wide-spread restrictions on public gatherings and community mobility, tourism largely ceased in March 2020. Early evidence on impacts on air travel, cruises, and accommodations have been devastating. While highly uncertain, early projections from UNWTO for 2020 suggest international arrivals could decline by 20 to 30% relative to 2019. Tourism is especially susceptible to measures to counteract pandemics because of restricted mobility and social distancing. The paper compares the impacts of COVID-19 to previous epidemic/pandemics and other types of global crises and explores how the pandemic may change society, the economy, and tourism. It discusses why COVID-19 is an analogue to the ongoing climate crisis, and why there is a need to question the volume growth tourism model advocated by UNWTO, ICAO, CLIA, WTTC and other tourism organizations.
Abstract
The novel coronavirus (COVID-19) is challenging the world. With no vaccine and limited medical capacity to treat the disease, nonpharmaceutical interventions (NPI) are the main strategy to contain the pandemic. Unprecedented global travel restrictions and stay-at-home orders are causing the most severe disruption of the global economy since World War II. With international travel bans affecting over 90% of the world population and wide-spread restrictions on public gatherings and community mobility, tourism largely ceased in March 2020. Early evidence on impacts on air travel, cruises, and accommodations have been devastating. While highly uncertain, early projections from UNWTO for 2020 suggest international arrivals could decline by 20 to 30% relative to 2019. Tourism is especially susceptible to measures to counteract pandemics because of restricted mobility and social distancing. The paper compares the impacts of COVID-19 to previous epidemic/pandemics and other types of global crises and explores how the pandemic may change society, the economy, and tourism. It discusses why COVID-19 is an analogue to the ongoing climate crisis, and why there is a need to question the volume growth tourism model advocated by UNWTO, ICAO, CLIA, WTTC and other tourism organizations.
Ik schop dit topic toch weer omhoog, er zijn recent ook weer veel publicaties uitgekomen die ook meer zorgvuldig zijn
Over Reproductiegetal en scholen
[ Bericht 1% gewijzigd door Momo op 02-11-2020 12:44:02 ]
Over Reproductiegetal en scholen
quote:The temporal association of introducing and lifting non-pharmaceutical interventions with the time-varying reproduction number (R) of SARS-CoV-2: a modelling study across 131 countries
Research in context
Evidence before this study
The time-varying reproduction number (R; also known as Rt), defined by the expected number of secondary cases arising from a primary case infected at time t, is a metric that describes viral transmission at the population level. An R value above 1 indicates a growing outbreak, and an R value below 1 indicates a shrinking outbreak. We searched PubMed, medRxiv, and bioRxiv for studies that reported the effects of introducing and lifting non-pharmaceutical interventions (NPIs) on R of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) published between Jan 1 and Aug 5, 2020, using the keywords “COVID-19”, “SARS-CoV-2”, “intervention”, and “transmission”. No language restriction was applied. Studies in China, Hong Kong, South Korea, Singapore, and many European countries showed that several NPIs, including school closure, physical distancing, and lockdown, could reduce R substantially to near or below 1. However, little is known about the effects on R following the relaxation of these NPIs.
Added value of this study
To the best of our knowledge, this study is the first to explicitly quantify the effects of both introducing and lifting individual NPIs on R over time. By linking a global dataset of country-level daily R values with a global dataset of country-level policies on NPIs, we modelled the change in R values (as R ratio) from day 1 to day 28 following the introduction and relaxation of eight individual NPIs among 131 countries. We found that reopening schools, lifting bans on public events, lifting bans on public gatherings of more than ten people, lifting requirements to stay at home, and lifting internal movement limits were associated with an increase in R of 11–25% on day 28 following the relaxation. However, the effects of introducing and lifting NPIs were not immediate; it took a median of 8 days (IQR 6–9) following the introduction of NPIs to observe 60% of their maximum reduction in R and even longer (17 days [14–20]) following the relaxation to observe 60% of the maximum increase in R. A similar delay in response to the introduction and relaxation of NPIs was also identified using Google mobility data. We compared four different candidates of composite NPIs that countries might consider in response to a possible resurgence of COVID-19.
Implications of all the available evidence
We quantified the change in transmission of SARS-CoV-2, as measured by R, following the introduction and relaxation of individual NPIs, and found a delay of 1–3 weeks in observing the effects of introducing and lifting these NPIs. These findings provide additional evidence that can inform policy-maker decisions on which NPIs to introduce or lift and when to expect a notable effect following the introduction or the relaxation.

[ Bericht 1% gewijzigd door Momo op 02-11-2020 12:44:02 ]
Over herinfectie
quote:Genomic evidence for reinfection with SARS-CoV-2: a case study
Summary
Background
The degree of protective immunity conferred by infection with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is currently unknown. As such, the possibility of reinfection with SARS-CoV-2 is not well understood. We describe an investigation of two instances of SARS-CoV-2 infection in the same individual.
Methods
A 25-year-old man who was a resident of Washoe County in the US state of Nevada presented to health authorities on two occasions with symptoms of viral infection, once at a community testing event in April, 2020, and a second time to primary care then hospital at the end of May and beginning of June, 2020. Nasopharyngeal swabs were obtained from the patient at each presentation and twice during follow-up. Nucleic acid amplification testing was done to confirm SARS-CoV-2 infection. We did next-generation sequencing of SARS-CoV-2 extracted from nasopharyngeal swabs. Sequence data were assessed by two different bioinformatic methodologies. A short tandem repeat marker was used for fragment analysis to confirm that samples from both infections came from the same individual.
Findings
The patient had two positive tests for SARS-CoV-2, the first on April 18, 2020, and the second on June 5, 2020, separated by two negative tests done during follow-up in May, 2020. Genomic analysis of SARS-CoV-2 showed genetically significant differences between each variant associated with each instance of infection. The second infection was symptomatically more severe than the first.
Interpretation
Genetic discordance of the two SARS-CoV-2 specimens was greater than could be accounted for by short-term in vivo evolution. These findings suggest that the patient was infected by SARS-CoV-2 on two separate occasions by a genetically distinct virus. Thus, previous exposure to SARS-CoV-2 might not guarantee total immunity in all cases. All individuals, whether previously diagnosed with COVID-19 or not, should take identical precautions to avoid infection with SARS-CoV-2. The implications of reinfections could be relevant for vaccine development and application.
Goed bezig Momo!quote:
Ik schop dit topic toch weer omhoog, er zijn recent ook weer veel publicaties uitgekomen die ook meer zorgvuldig zijn
Zijn er ondertussen, zes maanden na het laatste berichtje in dit topic (2 mei), al weer wat nieuwe (al dan niet peer-reviewed) studies gepubliceerd denk je?
Goed idee om ze hier te bundelen. Slecht (idee) dat we daar ooit mee gestopt zijn eigenlijk.
"The man who never alters his opinion is like standing water, and breeds reptiles of the mind." - William Blake, The Marriage of Heaven and Hell.
Genetisch component waarom sommige mensen in Europa heel ziek kunnen worden.quote:The major genetic risk factor for severe COVID-19 is inherited from Neanderthals
Abstract
A recent genetic association study1 identified a gene cluster on chromosome 3 as a risk locus for respiratory failure after infection with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). A separate study (COVID-19 Host Genetics Initiative)2 comprising 3,199 hospitalized patients with coronavirus disease 2019 (COVID-19) and control individuals showed that this cluster is the major genetic risk factor for severe symptoms after SARS-CoV-2 infection and hospitalization. Here we show that the risk is conferred by a genomic segment of around 50 kilobases in size that is inherited from Neanderthals and is carried by around 50% of people in south Asia and around 16% of people in Europe.
Effecten van Dexamethasone op covid-19 patientenquote:Dexamethasone in hospitalised patients with COVID-19: addressing uncertainties
The impressive results of the RECOVERY trial established that a moderate dose of dexamethasone (6 mg daily for 10 days) reduced mortality in hospitalised patients with COVID-19 and respiratory failure who required therapy with supplemental oxygen or mechanical ventilation.
The data also indicated that dexamethasone might increase mortality in hospitalised patients who were not receiving oxygen. This landmark trial and the subsequent practice guidelines from several academic and health organisations recommending dexamethasone use in patients with severe COVID-19 have changed clinical practice for hospitalised patients on supplemental oxygen or mechanical ventilation
These favourable findings are supported by three other trialsof glucocorticoids for COVID-19, which stopped enrolment in early June, 2020, when the RECOVERY trial results were released. Each of these trials showed some evidence of benefit, although none had completed enrolment. A prospective meta-analysis of these and other trials, totalling 1703 participants (1007 [59%] from the RECOVERY trial), confirmed a reduction in 28-day mortality (summary odds ratio [OR] 0·66, 95% CI 0·53–0·82; p<0·001), with minimal heterogeneity across studies.6
While confirming beneficial effects of corticosteroids for critically ill hospitalised patients with COVID-19, some unanswered questions and issues remain that deserve discussion and should be addressed in future research.
Effecten van Hydroxychloroquine op covid-19 patientenquote:Early Hydroxychloroquine but not Chloroquine use reduces ICU admission in COVID-19 patients
Highlights
•
After the global push for the use of Hydroxychloroquine and Chloroquine there is ongoing discussion about the effectivity of these drugs.
•
Findings of this observational study provide crucial data on a potential protective effect of Hydroxychloroquine in non-ICU, hospitalized COVID-19 patients.
•
Early treatment with HCQ on the first day of admission is associated with a reduced risk of 53% in transfer to the ICU for mechanical ventilation.
•
This protective effect was not observed for Chloroquine, therefore these drugs cannot be regarded as interchangeable.
Nou, dat werd tijd na die hele media hetze tegen hydroxychloroquine. Het ging velen die voor HCQ waren namelijk om het zo vroeg mogelijk toedienen ervan, maar daar was tot voor kort weinig onderzoek naar gedaan.quote:
[..]
Effecten van Hydroxychloroquine op covid-19 patienten
A Robin Redbreast in a Cage Puts all Heaven in a Rage.
Heb je het artikel gelezen? Dat hele zwart-wit verhaal van het werkt wel of niet. Het werkt alleen voor reductie ICU opnames, niet voor de sterftekans. Dat is een beetje de conclusie hier. Net als meerdere middelen die nu onderzocht zijn. Er zijn meerdere middelen die effectief lijken, maar er is geen wondermiddel dat zoveel beter is dan de rest. Sowieso dat gespam op social media toen omdat dit het wondermiddel zou zijn omdat 10 patiënten genezen waren in Limburg... Alleen maar goed dat er uitgebreid onderzoek naar is gedaan..quote:
[..]
Nou, dat werd tijd na die hele media hetze tegen hydroxychloroquine. Het ging velen die voor HCQ waren namelijk om het zo vroeg mogelijk toedienen ervan, maar daar was tot voor kort weinig onderzoek naar gedaan.
Ja i know, i know. Dat zwart-wit verhaal erger ik me ontzettend aan in de media.quote:
Heb je het artikel gelezen? Dat hele zwart-wit verhaal van het werkt wel of niet. Het werkt alleen voor reductie ICU opnames, niet voor de sterftekans.
A Robin Redbreast in a Cage Puts all Heaven in a Rage.
En een recent artikel over Remdesivir, ook geen wondermiddel.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7262788/
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7262788/
quote:Our data show that remdesivir was superior to placebo in shortening the time to recovery in adults who were hospitalized with Covid-19 and had evidence of lower respiratory tract infection.
quote:Race, Ethnicity, and Age Trends in Persons Who Died from COVID-19 — United States, May–August 2020
Summary
What is already known about this topic?
Persons aged ≥65 years and members of minority racial and ethnic groups are disproportionately represented among COVID-19–associated deaths.
What is added by this report?
Analysis of 114,411 COVID-19–associated deaths reported to National Vital Statistics System during May–August 2020, found that 51.3% of decedents were non-Hispanic White, 24.2% were Hispanic or Latino (Hispanic), and 18.7% were non-Hispanic Black. The percentage of Hispanic decedents increased from 16.3% in May to 26.4% in August.
What are the implications for public health practice?
These results can inform public health messaging and mitigation efforts focused on prevention and early detection of infection among disproportionately affected groups so as to minimize subsequent mortality.
quote:Physical distancing, face masks, and eye protection to prevent person-to-person transmission of SARS-CoV-2 and COVID-19: a systematic review and meta-analysis
Background
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) causes COVID-19 and is spread person-to-person through close contact. We aimed to investigate the effects of physical distance, face masks, and eye protection on virus transmission in health-care and non-health-care (eg, community) settings.
Methods
We did a systematic review and meta-analysis to investigate the optimum distance for avoiding person-to-person virus transmission and to assess the use of face masks and eye protection to prevent transmission of viruses. We obtained data for SARS-CoV-2 and the betacoronaviruses that cause severe acute respiratory syndrome, and Middle East respiratory syndrome from 21 standard WHO-specific and COVID-19-specific sources. We searched these data sources from database inception to May 3, 2020, with no restriction by language, for comparative studies and for contextual factors of acceptability, feasibility, resource use, and equity. We screened records, extracted data, and assessed risk of bias in duplicate. We did frequentist and Bayesian meta-analyses and random-effects meta-regressions. We rated the certainty of evidence according to Cochrane methods and the GRADE approach. This study is registered with PROSPERO, CRD42020177047.
Findings
Our search identified 172 observational studies across 16 countries and six continents, with no randomised controlled trials and 44 relevant comparative studies in health-care and non-health-care settings (n=25 697 patients). Transmission of viruses was lower with physical distancing of 1 m or more, compared with a distance of less than 1 m (n=10 736, pooled adjusted odds ratio [aOR] 0·18, 95% CI 0·09 to 0·38; risk difference [RD] −10·2%, 95% CI −11·5 to −7·5; moderate certainty); protection was increased as distance was lengthened (change in relative risk [RR] 2·02 per m; pinteraction=0·041; moderate certainty). Face mask use could result in a large reduction in risk of infection (n=2647; aOR 0·15, 95% CI 0·07 to 0·34, RD −14·3%, −15·9 to −10·7; low certainty), with stronger associations with N95 or similar respirators compared with disposable surgical masks or similar (eg, reusable 12–16-layer cotton masks; pinteraction=0·090; posterior probability >95%, low certainty). Eye protection also was associated with less infection (n=3713; aOR 0·22, 95% CI 0·12 to 0·39, RD −10·6%, 95% CI −12·5 to −7·7; low certainty). Unadjusted studies and subgroup and sensitivity analyses showed similar findings.
Interpretation
The findings of this systematic review and meta-analysis support physical distancing of 1 m or more and provide quantitative estimates for models and contact tracing to inform policy. Optimum use of face masks, respirators, and eye protection in public and health-care settings should be informed by these findings and contextual factors. Robust randomised trials are needed to better inform the evidence for these interventions, but this systematic appraisal of currently best available evidence might inform interim guidance.
Een studie over het in een vroeg stadium gebruiken van zink en lage dosering hydroxychloroquine
quote:COVID-19 outpatients: early risk-stratified treatment with zinc plus low-dose hydroxychloroquine and azithromycin: a retrospective case series study
Highlights
• First COVID-19 outpatient study based on risk stratification and early antiviral treatment at the beginning of the disease.
• Low-dose hydroxychloroquine combined with zinc and azithromycin was an effective therapeutic approach against COVID-19.
• Significantly reduced hospitalisation rates in the treatment group.
• Reduced mortality rates in the treatment group.
Ware Wijsheid Liefdevolle Vrede
Peaceful Warrior "What are you?" "This Moment"
Peaceful Warrior "What are you?" "This Moment"
One in five COVID-19 patients develop mental illness within 90 days - study
Many COVID-19 survivors are likely to be at greater risk of developing mental illness, psychiatrists said on Monday, after a large study found 20% of those infected with the coronavirus are diagnosed with a psychiatric disorder within 90 days.
Many COVID-19 survivors are likely to be at greater risk of developing mental illness, psychiatrists said on Monday, after a large study found 20% of those infected with the coronavirus are diagnosed with a psychiatric disorder within 90 days.
Dit is best wel een zorgwekkend resultaat.quote:Bidirectional associations between COVID-19 and psychiatric disorder: retrospective cohort studies of 62 354 COVID-19 cases in the USA
Background
Adverse mental health consequences of COVID-19, including anxiety and depression, have been widely predicted but not yet accurately measured. There are a range of physical health risk factors for COVID-19, but it is not known if there are also psychiatric risk factors. In this electronic health record network cohort study using data from 69 million individuals, 62 354 of whom had a diagnosis of COVID-19, we assessed whether a diagnosis of COVID-19 (compared with other health events) was associated with increased rates of subsequent psychiatric diagnoses, and whether patients with a history of psychiatric illness are at a higher risk of being diagnosed with COVID-19.
Methods
We used the TriNetX Analytics Network, a global federated network that captures anonymised data from electronic health records in 54 health-care organisations in the USA, totalling 69·8 million patients. TriNetX included 62 354 patients diagnosed with COVID-19 between Jan 20, and Aug 1, 2020. We created cohorts of patients who had been diagnosed with COVID-19 or a range of other health events. We used propensity score matching to control for confounding by risk factors for COVID-19 and for severity of illness. We measured the incidence of and hazard ratios (HRs) for psychiatric disorders, dementia, and insomnia, during the first 14 to 90 days after a diagnosis of COVID-19.
Findings
In patients with no previous psychiatric history, a diagnosis of COVID-19 was associated with increased incidence of a first psychiatric diagnosis in the following 14 to 90 days compared with six other health events (HR 2·1, 95% CI 1·8–2·5 vs influenza; 1·7, 1·5–1·9 vs other respiratory tract infections; 1·6, 1·4–1·9 vs skin infection; 1·6, 1·3–1·9 vs cholelithiasis; 2·2, 1·9–2·6 vs urolithiasis, and 2·1, 1·9–2·5 vs fracture of a large bone; all p<0·0001). The HR was greatest for anxiety disorders, insomnia, and dementia. We observed similar findings, although with smaller HRs, when relapses and new diagnoses were measured. The incidence of any psychiatric diagnosis in the 14 to 90 days after COVID-19 diagnosis was 18·1% (95% CI 17·6–18·6), including 5·8% (5·2–6·4) that were a first diagnosis. The incidence of a first diagnosis of dementia in the 14 to 90 days after COVID-19 diagnosis was 1·6% (95% CI 1·2–2·1) in people older than 65 years. A psychiatric diagnosis in the previous year was associated with a higher incidence of COVID-19 diagnosis (relative risk 1·65, 95% CI 1·59–1·71; p<0·0001). This risk was independent of known physical health risk factors for COVID-19, but we cannot exclude possible residual confounding by socioeconomic factors.
Interpretation
Survivors of COVID-19 appear to be at increased risk of psychiatric sequelae, and a psychiatric diagnosis might be an independent risk factor for COVID-19. Although preliminary, our findings have implications for clinical services, and prospective cohort studies are warranted.
quote:Age-specific mortality and immunity patterns of SARS-CoV-2
Estimating the size and infection severity of the SARS-CoV-2 epidemic is made challenging by inconsistencies in available data. The number of COVID-19 deaths is often used as a key indicator for the epidemic size, but observed deaths represent only a minority of all infections1,2. Additionally, the heterogeneous burden in nursing homes and variable reporting of deaths in elderly individuals can hamper direct comparisons across countries of the underlying level of transmission and mortality rates3. Here we use age-specific COVID-19 death data from 45 countries and the results of 22 seroprevalence studies to investigate the consistency of infection and fatality patterns across multiple countries. We find that the age distribution of deaths in younger age groups (<65 years) is very consistent across different settings and demonstrate how this data can provide robust estimates of the share of the population that has been infected. We estimate that the infection-to-fatality ratio (IFR) is lowest among 5-9 years old, with a log-linear increase by age among individuals older than 30 years. Population age-structures and heterogeneous burdens in nursing homes explain some but not all of the heterogeneity between countries in infection-fatality ratios. Among the 45 countries included in our analysis, we estimate approximately 5% of these populations had been infected by the 1st of September 2020, with much higher transmission likely to have occurred in a number of Latin American countries. This simple modelling framework can help countries assess the progression of the pandemic and can be applied wherever reliable age-specific death data exists.
quote:Mobility network models of COVID-19 explain inequities and inform reopening
The COVID-19 pandemic dramatically changed human mobility patterns, necessitating epidemiological models which capture the effects of changes in mobility on virus spread1. We introduce a metapopulation SEIR model that integrates fine-grained, dynamic mobility networks to simulate the spread of SARS-CoV-2 in 10 of the largest US metropolitan statistical areas. Derived from cell phone data, our mobility networks map the hourly movements of 98 million people from neighborhoods (census block groups, or CBGs) to points of interest (POIs) such as restaurants and religious establishments, connecting 57k CBGs to 553k POIs with 5.4 billion hourly edges. We show that by integrating these networks, a relatively simple SEIR model can accurately fit the real case trajectory, despite substantial changes in population behavior over time. Our model predicts that a small minority of “superspreader” POIs account for a large majority of infections and that restricting maximum occupancy at each POI is more effective than uniformly reducing mobility. Our model also correctly predicts higher infection rates among disadvantaged racial and socioeconomic groups2–8 solely from differences in mobility: we find that disadvantaged groups have not been able to reduce mobility as sharply, and that the POIs they visit are more crowded and therefore higher-risk. By capturing who is infected at which locations, our model supports detailed analyses that can inform more effective and equitable policy responses to COVID-19.
Geen goed nieuws voor horeca, maar aan de andere kant... als je ziet waar ze het tegen afgezet hebben: tankstations en vooral heel veel winkels.
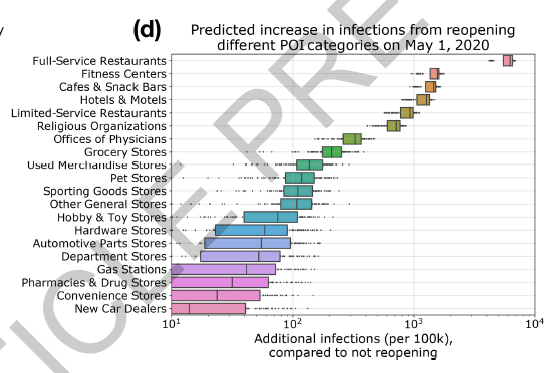
Jammer dat scholen, universiteiten, festivals, concerten, grote sportevenementen als toeschouwer en deelnemer er niet tussen staan. Maar goed, de meeste van die dingen hebben ook niet plaatsgevonden het afgelopen half jaar.


quote:The 40 health systems, COVID-19 (40HS, C-19) study
Background
The health, social and economic consequences of the severe acute respiratory syndrome coronavirus (SARS-CoV-2, henceforth COVID-19) pandemic have loomed large as every national government made decisions about how to respond. The 40 Health Systems, COVID-19 (40HS, C-19) study aimed to investigate relationships between governments’ capacity to respond (CTR), their response stringency, scope of COVID-19 testing and COVID-19 outcomes.
Methods
Data over March and April 2020 were extracted for 40 national health systems on prepandemic government CTR (Global Competitiveness Index), stringency measures (Oxford COVID-19 Government Response Tracker Stringency Index), approach to COVID-19 testing and COVID-19 cases and deaths (Our-World-in-Data). Multidimensional scaling (MDS) and cluster analysis were applied to examine latent dimensions and visualize country similarities and dissimilarities. Outcomes were tested using multivariate and one-way analyses of variances and Kruskal–Wallis H tests.
Results
The MDS model found three dimensions explaining 91% of the variance and cluster analysis identified five national groupings. There was no association between national governments’ prepandemic CTR and the adoption of early stringent public health measures or approach to COVID-19 testing. Two national clusters applied early stringency measures and reported significantly lower cumulative deaths. The best performing national cluster (comprising Australia, South Korea, Iceland and Taiwan) adopted relatively early stringency measures but broader testing earlier than others, which was associated with a change in disease trajectory and the lowest COVID-19 death rates. Two clusters (one with high CTR and one low) both adopted late stringency measures and narrow testing and performed least well in COVID-19 outcomes.
Conclusion
Early stringency measures and intrinsic national capacities to deal with a pandemic are insufficient. Extended stringency measures, important in the short term, are not economically sustainable. Broad-based testing is key to managing COVID-19.
quote:Transmission of SARS-CoV-2 on mink farms between humans and mink and back to humans
Abstract
Animal experiments have shown that non-human primates, cats, ferrets, hamsters, rabbits and bats can be infected by SARS-CoV-2. In addition, SARS-CoV-2 RNA has been detected in felids, mink and dogs in the field. Here, we describe an in-depth investigation using whole genome sequencing of outbreaks on 16 mink farms and the humans living or working on these farms. We conclude that the virus was initially introduced from humans and has since evolved, most likely reflecting widespread circulation among mink in the beginning of the infection period several weeks prior to detection. Despite enhanced biosecurity, early warning surveillance and immediate culling of infected farms, transmission occurred between mink farms in three big transmission clusters with unknown modes of transmission. Sixty-eight percent (68%) of the tested mink farm residents, employees and/or contacts had evidence of SARS-CoV-2 infection. Where whole genomes were available, these persons were infected with strains with an animal sequence signature, providing evidence of animal to human transmission of SARS-CoV-2 within mink farms.
quote:Persistence and Evolution of SARS-CoV-2 in an Immunocompromised Host
The coronavirus can mutate swiftly in one person’s body
The new coronavirus resurged again and again in the body of an infected man, eventually killing him while showing evidence of fast-paced evolution.
Manuela Cernadas and Jonathan Li at Brigham and Women’s Hospital in Boston, Massachusetts, and their colleagues followed the course of COVID-19 in a 45-year-old man with a long-standing autoimmune disorder, who was on a medication regimen that included powerful immunosuppressants (B. Choi et al. N. Engl. J. Med. https://doi.org/fhv8; 2020). Roughly 40 days after the man first tested positive for SARS-CoV-2, follow-up tests indicated that the virus was dwindling — but it surged back, despite antiviral treatment.
The man’s infection subsided and then returned twice more before he died, five months after his first COVID-19 diagnosis. Genomic analysis showed that the man had not been infected multiple times. Instead, the virus had lingered and quickly mutated in his body.
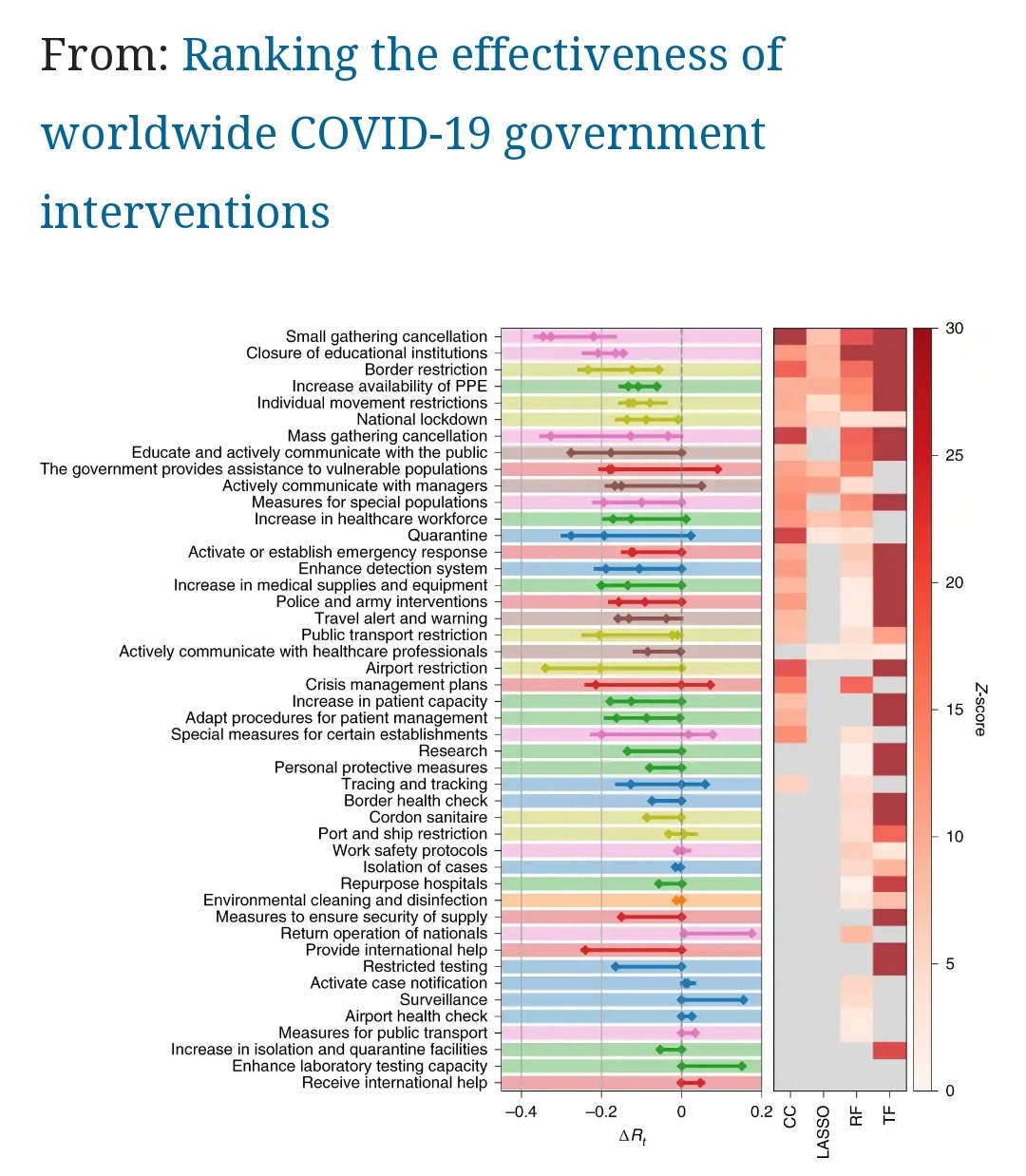
quote:Ranking the effectiveness of worldwide COVID-19 government interventions
Assessing the effectiveness of non-pharmaceutical interventions (NPIs) to mitigate the spread of SARS-CoV-2 is critical to inform future preparedness response plans. Here we quantify the impact of 6,068 hierarchically coded NPIs implemented in 79 territories on the effective reproduction number, Rt, of COVID-19. We propose a modelling approach that combines four computational techniques merging statistical, inference and artificial intelligence tools. We validate our findings with two external datasets recording 42,151 additional NPIs from 226 countries. Our results indicate that a suitable combination of NPIs is necessary to curb the spread of the virus. Less disruptive and costly NPIs can be as effective as more intrusive, drastic, ones (for example, a national lockdown). Using country-specific ‘what-if’ scenarios, we assess how the effectiveness of NPIs depends on the local context such as timing of their adoption, opening the way for forecasting the effectiveness of future interventions
(Gedeeltelijke) immuniteit lijkt wel lang te zijn. Misschien kan iemand met een medische/biologische achtergrond hier meer achtergrond bij geven?quote:Immunological memory to SARS-CoV-2 assessed for greater than six months after infection
Abstract
Understanding immune memory to SARS-CoV-2 is critical for improving diagnostics and vaccines, and for assessing the likely future course of the pandemic. We analyzed multiple compartments of circulating immune memory to SARS-CoV-2 in 185 COVID-19 cases, including 41 cases at > 6 months post-infection. Spike IgG was relatively stable over 6+ months. Spike-specific memory B cells were more abundant at 6 months than at 1 month. SARS-CoV-2-specific CD4+ T cells and CD8+ T cells declined with a half-life of 3-5 months. By studying antibody, memory B cell, CD4+ T cell, and CD8+ T cell memory to SARS-CoV-2 in an integrated manner, we observed that each component of SARS-CoV-2 immune memory exhibited distinct kinetics.
Competing Interest Statement
A.S. is a consultant for Gritstone, Flow Pharma, Merck, Epitogenesis, Gilead and Avalia. S.C. is a consultant for Avalia. LJI has filed for patent protection for various aspects of T cell epitope and vaccine design work. Mount Sinai has licensed serological assays to commercial entities and has filed for patent protection for serological assays. D.S., F.A., V.S. and F.K. are listed as inventors on the pending patent application (F.K., V.S.), and Newcastle disease virus (NDV)-based SARS-CoV-2 vaccines that name F.K. as inventor. All other authors declare no conflict of interest.
Ik weet ook niet hoe dat allemaal zit, maar wat ik ervan lees is dat het ook moeilijk te bepalen is door levels van antistoffen of T-cellen of activiteit van T-cellen te meten. Er moet een relatie zijn, maar die is erg lastig te bepalen.
De effectiviteit van een vaccin zal over de loop van tijd afnemen, het is niet zo dat het de ene dag 95% werkt en de volgende dag 0%. En bescherming kan zich ook op verschillende manieren uiten.
Krijg je geen symptomen en ben je niet besmettelijk.
Krijg je wel symptomen maar alleen licht en ben je niet besmettelijk.
Krijg je wel symptomen en ben je besmettelijk, maar raak je niet ziek.
Word je misschien wel ziek, maar minder ziek, etc.
En dat beeld zal over de loop van tijd ook varieren. Tot dusver lijken vaccins in ieder geval in het begin heel goed te werken, dus als hun werkzaamheid gedurende de tijd afneemt, dan is het beginpunt in ieder geval goed.
De effectiviteit van een vaccin zal over de loop van tijd afnemen, het is niet zo dat het de ene dag 95% werkt en de volgende dag 0%. En bescherming kan zich ook op verschillende manieren uiten.
Krijg je geen symptomen en ben je niet besmettelijk.
Krijg je wel symptomen maar alleen licht en ben je niet besmettelijk.
Krijg je wel symptomen en ben je besmettelijk, maar raak je niet ziek.
Word je misschien wel ziek, maar minder ziek, etc.
En dat beeld zal over de loop van tijd ook varieren. Tot dusver lijken vaccins in ieder geval in het begin heel goed te werken, dus als hun werkzaamheid gedurende de tijd afneemt, dan is het beginpunt in ieder geval goed.
https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(20)32466-1/fulltext
En een press release over dezelfde studie: https://covid19vaccinetrial.co.uk/phase-ii-trial-publicationquote:Interpretation
ChAdOx1 nCoV-19 appears to be better tolerated in older adults than in younger adults and has similar immunogenicity across all age groups after a boost dose. Further assessment of the efficacy of this vaccine is warranted in all age groups and individuals with comorbidities.
Zijn dit soort studies ook bekend van Moderna en Pfizer?quote:
https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(20)32466-1/fulltext
[..]
En een press release over dezelfde studie: https://covid19vaccinetrial.co.uk/phase-ii-trial-publication
Die hebben wel allebei een fase II studie gepubliceerd, maar geen follow up met de focus op hogere leeftijdsklassen. Al melde Pfizer gister wel dat het daar ook effectief was. Vanwege de betrokkenheid van de Universiteit van Oxford bij het Oxford/AstraZeneca vaccin is er een grotere push vanuit het project (onderzoek) zelf om wetenschappelijk te publiceren. In ieder geval ten opzichte van de meer commercieel gefocuste andere studies, die minder betrokkenheid van universiteiten hebben.
Goed nieuws over herinfectie kansquote:Antibodies to SARS-CoV-2 are associated with protection against reinfection
Background It is critical to understand whether infection with Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) protects from subsequent reinfection. Methods We investigated the incidence of SARS-CoV-2 PCR-positive results in seropositive and seronegative healthcare workers (HCWs) attending asymptomatic and symptomatic staff testing at Oxford University Hospitals, UK. Baseline antibody status was determined using anti-spike and/or anti-nucleocapsid IgG assays and staff followed for up to 30 weeks. We used Poisson regression to estimate the relative incidence of PCR-positive results and new symptomatic infection by antibody status, accounting for age, gender and changes in incidence over time. Results A total of 12219 HCWs participated and had anti-spike IgG measured, 11052 were followed up after negative and 1246 after positive antibody results including 79 who seroconverted during follow up. 89 PCR-confirmed symptomatic infections occurred in seronegative individuals (0.46 cases per 10,000 days at risk) and no symptomatic infections in those with anti-spike antibodies. Additionally, 76 (0.40/10,000 days at risk) anti-spike IgG seronegative individuals had PCR-positive tests in asymptomatic screening, compared to 3 (0.21/10,000 days at risk) seropositive individuals. Overall, positive baseline anti-spike antibodies were associated with lower rates of PCR-positivity (with or without symptoms) (adjusted rate ratio 0.24 [95%CI 0.08-0.76, p=0.015]). Rate ratios were similar using anti-nucleocapsid IgG alone or combined with anti-spike IgG to determine baseline status. Conclusions Prior SARS-CoV-2 infection that generated antibody responses offered protection from reinfection for most people in the six months following infection. Further work is required to determine the long-term duration and correlates of post-infection immunity.
Minder goed nieuws over herinfectiekans en dus ook voor de lange-termijn-effectiviteit van vaccins:
Dit betreft een onderzoek naar verkoudheidssvirussen in 513 serum samples afkomstig uit de Amsterdam Cohort Studies on HIV infection
https://www.nature.com/articles/s41591-020-1083-1
A key unsolved question in the current coronavirus disease 2019 (COVID-19) pandemic is the duration of acquired immunity. Insights from infections with the four seasonal human coronaviruses might reveal common characteristics applicable to all human coronaviruses. We monitored healthy individuals for more than 35 years and determined that reinfection with the same seasonal coronavirus occurred frequently at 12 months after infection.
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is a novel coronavirus responsible for an ongoing pandemic. To date, there is limited evidence of reinfection by SARS-CoV-2, although it is generally assumed that reinfections by coronaviruses occur. To prepare for future waves of Coronavirus Disease 2019 (COVID-19), it is important to elucidate the duration of protection to reinfection for which the seasonal coronaviruses might serve as an informative model. There are four species of seasonal coronaviruses—HCoV-NL63, HCoV-229E, HCoV-OC43 and HCoV-HKU1—that all can cause respiratory tract infections but are otherwise genetically and biologically dissimilar. They belong to two distinct taxonomic genera and use different receptor molecules with varying host cell tropism1. Given this large variation, we hypothesize that characteristics shared by these four seasonal coronaviruses, such as the duration of protective immunity, are representative of all human coronaviruses, including SARS-CoV-2. Therefore, the aim of this study was to investigate the duration of protection from seasonal coronavirus reinfections.
We show that reinfections by natural infection occur for all four seasonal coronaviruses, suggesting that it is a common feature for all human coronaviruses, including SARS-CoV-2. Reinfections occurred most frequently at 12 months after infection, indicating that protective immunity is only short-lived.
Dit betreft een onderzoek naar verkoudheidssvirussen in 513 serum samples afkomstig uit de Amsterdam Cohort Studies on HIV infection
https://www.nature.com/articles/s41591-020-1083-1
A key unsolved question in the current coronavirus disease 2019 (COVID-19) pandemic is the duration of acquired immunity. Insights from infections with the four seasonal human coronaviruses might reveal common characteristics applicable to all human coronaviruses. We monitored healthy individuals for more than 35 years and determined that reinfection with the same seasonal coronavirus occurred frequently at 12 months after infection.
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is a novel coronavirus responsible for an ongoing pandemic. To date, there is limited evidence of reinfection by SARS-CoV-2, although it is generally assumed that reinfections by coronaviruses occur. To prepare for future waves of Coronavirus Disease 2019 (COVID-19), it is important to elucidate the duration of protection to reinfection for which the seasonal coronaviruses might serve as an informative model. There are four species of seasonal coronaviruses—HCoV-NL63, HCoV-229E, HCoV-OC43 and HCoV-HKU1—that all can cause respiratory tract infections but are otherwise genetically and biologically dissimilar. They belong to two distinct taxonomic genera and use different receptor molecules with varying host cell tropism1. Given this large variation, we hypothesize that characteristics shared by these four seasonal coronaviruses, such as the duration of protective immunity, are representative of all human coronaviruses, including SARS-CoV-2. Therefore, the aim of this study was to investigate the duration of protection from seasonal coronavirus reinfections.
We show that reinfections by natural infection occur for all four seasonal coronaviruses, suggesting that it is a common feature for all human coronaviruses, including SARS-CoV-2. Reinfections occurred most frequently at 12 months after infection, indicating that protective immunity is only short-lived.
"Leuker kunnen wij het niet maken , ingewikkelder wel." Lang leve de Belastingdienst!
quote:The effect of temperature and humidity on the stability of SARS-CoV-2 and other enveloped viruses
Abstract
Understanding the impact of environmental conditions on virus viability and transmission potential is crucial to anticipating epidemic dynamics and designing mitigation strategies. Ambient temperature and humidity are known to have strong effects on the environmental stability of viruses, but a general quantitative understanding of how temperature and humidity affect virus stability has remained elusive. We characterize the stability of SARS-CoV-2 on an inert surface at a variety of temperature and humidity conditions, and introduce a mechanistic model that enables accurate prediction of virus stability in unobserved conditions. We find that SARS-CoV-2 survives better at low temperatures and extreme relative humidities; median estimated virus half-life was more than 24 hours at 10 °C and 40 % RH, but approximately an hour and a half at 27 °C and 65 % RH. Moreover, our model predicts observations from other human coronaviruses and other studies of SARS-CoV-2, suggesting the existence of shared mechanisms that determine environmental stability across a number of enveloped viruses. Our results highlight scenarios of particular transmission risk and point to broad strategies for pandemic mitigation, while opening new frontiers for the mechanistic study of viral transmission.
Nieuwe Chinese studie laat zien dat asymptomatische gevallen niet besmettelijk zijn.
https://www.nature.com/articles/s41467-020-19802-w
https://www.nature.com/articles/s41467-020-19802-w
quote:All close contacts of the asymptomatic positive cases tested negative, indicating that the asymptomatic positive cases detected in this study were unlikely to be infectious.
quote:In summary, the detection rate of asymptomatic positive cases in the post-lockdown Wuhan was very low (0.303/10,000), and there was no evidence that the identified asymptomatic positive cases were infectious.
Goed nieuws! Al is het natuurlijk ook een sliding scale: Hoe meer symptomen hoe hoger je virus load waarschijnlijk, en hoe hoger de kans dat je iemand anders kunt besmetten. Maar je kunt zoiets wel bedenken, om er zeker van te zijn moet er onderzoek naar gedaan worden om zoiets te bevestigen of weerleggen. Top dat dat gedaan is!
Het coronavirus is niet gemuteerd naar een meer besmetbare variant.quote:No evidence for increased transmissibility from recurrent mutations in SARS-CoV-2
COVID-19 is caused by the coronavirus SARS-CoV-2, which jumped into the human population in late 2019 from a currently uncharacterised animal reservoir. Due to this recent association with humans, SARS-CoV-2 may not yet be fully adapted to its human host. This has led to speculations that SARS-CoV-2 may be evolving towards higher transmissibility. The most plausible mutations under putative natural selection are those which have emerged repeatedly and independently (homoplasies). Here, we formally test whether any homoplasies observed in SARS-CoV-2 to date are significantly associated with increased viral transmission. To do so, we develop a phylogenetic index to quantify the relative number of descendants in sister clades with and without a specific allele. We apply this index to a curated set of recurrent mutations identified within a dataset of 46,723 SARS-CoV-2 genomes isolated from patients worldwide. We do not identify a single recurrent mutation in this set convincingly associated with increased viral transmission. Instead, recurrent mutations currently in circulation appear to be evolutionary neutral and primarily induced by the human immune system via RNA editing, rather than being signatures of adaptation. At this stage we find no evidence for significantly more transmissible lineages of SARS-CoV-2 due to recurrent mutations.
Hadden ze daar al de mutatie in fretten in Denemarken bij meegenomen?
Hier een artikel over viral load and shedding. Take home message:
Hier een artikel over viral load and shedding. Take home message:
https://www.thelancet.com/journals/lanmic/article/PIIS2666-5247(20)30172-5/fulltextquote:No study detected live virus beyond day 9 of illness, despite persistently high viral loads, which were inferred from cycle threshold values.
Wel opmerkelijk dat de piek van SARS-Cov-2 eerder is dan de pieken van SARS-Cov en MERS-Cov, terwijl SARS-Cov-2 wel besmettelijker is. Ik had verwacht dat SARS-Cov-2 langer besmettelijk zou zijn. Misschien gaat bij SARS-Cov-2 de piek viral shedding meer vooraf aan de symptomen, omdat het zo snel op komt zetten? Dus je bent besmettelijk voor je er erg in hebt, terwijl je bij SARS-CoV en MERS-CoV pas echt besmettelijk werd na het ontwikkelen van symptomen.quote:Findings
79 studies (5340 individuals) on SARS-CoV-2, eight studies (1858 individuals) on SARS-CoV, and 11 studies (799 individuals) on MERS-CoV were included. Mean duration of SARS-CoV-2 RNA shedding was 17·0 days (95% CI 15·5–18·6; 43 studies, 3229 individuals) in upper respiratory tract, 14·6 days (9·3–20·0; seven studies, 260 individuals) in lower respiratory tract, 17·2 days (14·4–20·1; 13 studies, 586 individuals) in stool, and 16·6 days (3·6–29·7; two studies, 108 individuals) in serum samples. Maximum shedding duration was 83 days in the upper respiratory tract, 59 days in the lower respiratory tract, 126 days in stools, and 60 days in serum. Pooled mean SARS-CoV-2 shedding duration was positively associated with age (slope 0·304 [95% CI 0·115–0·493]; p=0·0016). No study detected live virus beyond day 9 of illness, despite persistently high viral loads, which were inferred from cycle threshold values. SARS-CoV-2 viral load in the upper respiratory tract appeared to peak in the first week of illness, whereas that of SARS-CoV peaked at days 10–14 and that of MERS-CoV peaked at days 7–10.
Over het dragen van maskers.
https://msphere.asm.org/content/5/5/e00637-20
https://msphere.asm.org/content/5/5/e00637-20
quote:Guidelines from the CDC and the WHO recommend the wearing of face masks to prevent the spread of coronavirus (CoV) disease 2019 (COVID-19); however, the protective efficiency of such masks against airborne transmission of infectious severe acute respiratory syndrome CoV-2 (SARS-CoV-2) droplets/aerosols is unknown. Here, we developed an airborne transmission simulator of infectious SARS-CoV-2-containing droplets/aerosols produced by human respiration and coughs and assessed the transmissibility of the infectious droplets/aerosols and the ability of various types of face masks to block the transmission. We found that cotton masks, surgical masks, and N95 masks all have a protective effect with respect to the transmission of infective droplets/aerosols of SARS-CoV-2 and that the protective efficiency was higher when masks were worn by a virus spreader. Importantly, medical masks (surgical masks and even N95 masks) were not able to completely block the transmission of virus droplets/aerosols even when completely sealed. Our data will help medical workers understand the proper use and performance of masks and determine whether they need additional equipment to protect themselves from infected patients.
IMPORTANCE
Airborne simulation experiments showed that cotton masks, surgical masks, and N95 masks provide some protection from the transmission of infective SARS-CoV-2 droplets/aerosols; however, medical masks (surgical masks and even N95 masks) could not completely block the transmission of virus droplets/aerosols even when sealed.
Verspreiding door kinderen belangrijker dan gedacht.
https://www.princeton.edu/news/2020/09/30/largest-covid-19-contact-tracing-study-date-finds-children-key-spread-evidence
https://science.sciencemag.org/content/370/6517/691
https://www.princeton.edu/news/2020/09/30/largest-covid-19-contact-tracing-study-date-finds-children-key-spread-evidence
https://science.sciencemag.org/content/370/6517/691
quote:The researchers found that the chances of a person with coronavirus, regardless of their age, passing it on to a close contact ranged from 2.6% in the community to 9% in the household. The researchers found that children and young adults — who made up one-third of COVID cases — were especially key to transmitting the virus in the studied populations.
“Kids are very efficient transmitters in this setting, which is something that hasn’t been firmly established in previous studies,” Laxminarayan said. “We found that reported cases and deaths have been more concentrated in younger cohorts than we expected based on observations in higher-income countries.”
quote:Effectiveness of face masks for the population
Background: Health authorities and organizations consider non-medical face masks as an additional passive means to prevent virus diffusion. Communication strategies disseminate information among the population that such masks are essential for mitigating virus diffusion. However, scientific studies are not conclusive in showing the undisputed filtration efficiency of fabric/cloth facial masks (both commercial and homemade).
Objectives: This study examines scientific data about the effectiveness of face masks before and during the COVID-19 emergency. Present trends in the making of commercial and homemade fabric/cloth face masks are also examined.
Methods: Statistical data of published studies are analyzed and compared. Main considerations and suggestions are also extracted and discussed. Current approaches are examined for assessing the characteristics and effectiveness of fabric/cloth commercial and homemade face masks intended for the population.
Result: Conflicting data exist as to whether non-medical masks have a protective effect from the spread of respiratory viruses. Both medical masks (MDs) and respiratory personal protection equipment (PPE) show a given effectiveness value.
Conclusion: Concerning commercial and homemade fabric/cloth masks, giving general indications on the choice of materials and their assemblage is difficult as it is not possible to assess the effectiveness of the filter media with respect to the kind of multiphase fluid that may be emitted upon breathing, sneezing, or coughing under different environmental conditions. This is particularly important because airflow rate, temperature, humidity, and duration of use will affect the performance of filter media. Moreover, while a mask may have excellent filter media, droplets may leak into the face-piece unless there is an adequate facial seal. In the presence of leaks, any type of mask may actually offer less protection independently of its nominal filtering effìciency.
Nederlands onderzoek naar de effect van scholen op het reproductiegetal. Conclusie is dat scholen wel significant bijdragen.quote:Model-based evaluation of school- and non-school-related measures to control the COVID-19 pandemic
Background In autumn 2020, many countries, including the Netherlands, are experiencing a second wave of the COVID-19 pandemic. Health policymakers are struggling with choosing the right mix of measures to keep the COVID-19 case numbers under control, but still allow a minimum of social and economic activity. The priority to keep schools open is high, but the role of school-based contacts in the epidemiology of SARS-CoV-2 is incompletely understood. We used a transmission model to estimate the impact of school contacts on transmission of SARS-CoV-2 and to assess the effects of school-based measures, including school closure, on controlling the pandemic at different time points during the pandemic.
Methods and Findings The age-structured model was fitted to age-specific seroprevalence and hospital admission data from the Netherlands during spring 2020. Compared to adults older than 60 years, the estimated susceptibility was 23% (95%CrI 20—28%) for children aged 0 to 20 years and 61% (95%CrI 50%—72%) for the age group of 20 to 60 years. The time points considered in the analyses were August 2020 when the effective reproduction number (Re) was estimated to be 1.31 (95%CrI 1.15—2.07), schools just opened after the summer holidays and measures were reinforced with the aim to reduce Re to a value below 1, and (ii) November 2020 when measures had reduced Re to 1.00 (95%CrI 0.94—1.33). In this period schools remained open. Our model predicts that keeping schools closed after the summer holidays, in the absence of other measures, would have reduced Re by 10% (from 1.31 to 1.18 (95%CrI 1.04—1.83)) and thus would not have prevented the second wave in autumn 2020. Reducing non-school-based contacts in August 2020 to the level observed during the first wave of the pandemic would have reduced Re to 0.83 (95%CrI 0.75—1.10). Yet, this reduction was not achieved and the observed Re in November was 1.00. Our model predicts that closing schools in November 2020 could reduce Re from the observed value of 1.00 to 0.84 (95%CrI 0.81—0.90), with unchanged non-school based contacts. Reductions in Re due to closing schools in November 2020 were 8% for 10 to 20 years old children, 5% for 5 to 10 years old children and negligible for 0 to 5 years old children.
Conclusions The impact of measures reducing school-based contacts, including school closure, depends on the remaining opportunities to reduce non-school-based contacts. If opportunities to reduce Re with non-school-based measures are exhausted or undesired and Re is still close to 1, the additional benefit of school-based measures may be considerable, particularly among the older school children
Niet peer-reviewed maar wel intressant onderzoekquote:Exclusive: Kids catch and spread coronavirus half as much as adults, Iceland study confirms
Big decisions around COVID-19 and children have been heavy on politics and short on science. New large-scale studies are changing that.
“They can and do get infected and transmit to others, but they do both less frequently than adults,” says Kári Stefánsson, the chief executive of deCODE.
Nog een artikel over restaurants, dit laat ook weer zien waarom veel landen er voor kiezen om restaurants (gedeeltelijk) te sluitenquote:Evidence of Long-Distance Droplet Transmission of SARS-CoV-2 by Direct Air Flow in a Restaurant in Korea
Abstract
Background
The transmission mode of severe acute respiratory syndrome coronavirus 2 is primarily known as droplet transmission. However, a recent argument has emerged about the possibility of airborne transmission. On June 17, there was a coronavirus disease 2019 (COVID-19) outbreak in Korea associated with long distance droplet transmission.
Methods
The epidemiological investigation was implemented based on personal interviews and data collection on closed-circuit television images, and cell phone location data. The epidemic investigation support system developed by the Korea Disease Control and Prevention Agency was used for contact tracing. At the restaurant considered the site of exposure, air flow direction and velocity, distances between cases, and movement of visitors were investigated.
Results
A total of 3 cases were identified in this outbreak, and maximum air flow velocity of 1.2 m/s was measured between the infector and infectee in a restaurant equipped with ceiling-type air conditioners. The index case was infected at a 6.5 m away from the infector and 5 minutes exposure without any direct or indirect contact.
Conclusion
Droplet transmission can occur at a distance greater than 2 m if there is direct air flow from an infected person. Therefore, updated guidelines involving prevention, contact tracing, and quarantine for COVID-19 are required for control of this highly contagious disease.
Over het effect van maatregelen in verschillende landenquote:Inferring the effectiveness of government interventions against COVID-19
Abstract
Governments are attempting to control the COVID-19 pandemic with nonpharmaceutical interventions (NPIs). However, the effectiveness of different NPIs at reducing transmission is poorly understood. We gathered chronological data on the implementation of NPIs for several European, and other, countries between January and the end of May 2020. We estimate the effectiveness of NPIs, ranging from limiting gathering sizes, business closures, and closure of educational institutions to stay-at-home orders. To do so, we used a Bayesian hierarchical model that links NPI implementation dates to national case and death counts and supported the results with extensive empirical validation. Closing all educational institutions, limiting gatherings to 10 people or less, and closing face-to-face businesses each reduced transmission considerably. The additional effect of stay-at-home orders was comparatively small.

Let op in dit plaatje staat reduction, dus hoe hoger het getal, hoe meer daling van het reproductiegetal.
quote:Dynamic Change of COVID-19 Seroprevalence among Asymptomatic Population in Tokyo during the Second Wave
Conclusions and Relevance: COVID-19 infection may have spread widely across the general population of Tokyo despite the very low fatality rate. Given the temporal correlation between the rise in seropositivity and the decrease in reported COVID-19 cases that occurred without a shut-down, herd immunity may be implicated.
Nog twee artikelen van de Oxford studie die vandeweek gepubliceerd zijn.
T cell and antibody responses induced by a single dose of ChAdOx1 nCoV-19 (AZD1222) vaccine in a phase 1/2 clinical trial.
T cell and antibody responses induced by a single dose of ChAdOx1 nCoV-19 (AZD1222) vaccine in a phase 1/2 clinical trial.
En: Phase 1/2 trial of SARS-CoV-2 vaccine ChAdOx1 nCoV-19 with a booster dose induces multifunctional antibody responsesquote:Abstract
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), the causative agent of Coronavirus Disease 2019 (COVID-19), has caused a global pandemic, and safe, effective vaccines are urgently needed. Strong, Th1-skewed T cell responses can drive protective humoral and cell-mediated immune responses and might reduce the potential for disease enhancement. Cytotoxic T cells clear virus-infected host cells and contribute to control of infection. Studies of patients infected with SARS-CoV-2 have suggested a protective role for both humoral and cell-mediated immune responses in recovery from COVID-19. ChAdOx1 nCoV-19 (AZD1222) is a candidate SARS-CoV-2 vaccine comprising a replication-deficient simian adenovirus expressing full-length SARS-CoV-2 spike protein. We recently reported preliminary safety and immunogenicity data from a phase 1/2 trial of the ChAdOx1 nCoV-19 vaccine (NCT04400838)7 given as either a one- or two-dose regimen. The vaccine was tolerated, with induction of neutralizing antibodies and antigen-specific T cells against the SARS-CoV-2 spike protein. Here we describe, in detail, exploratory analyses of the immune responses in adults, aged 18–55 years, up to 8 weeks after vaccination with a single dose of ChAdOx1 nCoV-19 in this trial, demonstrating an induction of a Th1-biased response characterized by interferon-γ and tumor necrosis factor-α cytokine secretion by CD4+ T cells and antibody production predominantly of IgG1 and IgG3 subclasses. CD8+ T cells, of monofunctional, polyfunctional and cytotoxic phenotypes, were also induced. Taken together, these results suggest a favorable immune profile induced by ChAdOx1 nCoV-19 vaccine, supporting the progression of this vaccine candidate to ongoing phase 2/3 trials to assess vaccine efficacy.
quote:Abstract
More than 190 vaccines are currently in development to prevent infection by the novel severe acute respiratory syndrome coronavirus 2. Animal studies suggest that while neutralizing antibodies against the viral spike protein may correlate with protection, additional antibody functions may also be important in preventing infection. Previously, we reported early immunogenicity and safety outcomes of a viral vector coronavirus vaccine, ChAdOx1 nCoV-19 (AZD1222), in a single-blinded phase 1/2 randomized controlled trial of healthy adults aged 18–55 years (NCT04324606). Now we describe safety and exploratory humoral and cellular immunogenicity of the vaccine, from subgroups of volunteers in that trial, who were subsequently allocated to receive a homologous full-dose (SD/SD D56; n = 20) or half-dose (SD/LD D56; n = 32) ChAdOx1 booster vaccine 56 d following prime vaccination. Previously reported immunogenicity data from the open-label 28-d interval prime-boost group (SD/SD D28; n = 10) are also presented to facilitate comparison. Additionally, we describe volunteers boosted with the comparator vaccine (MenACWY; n = 10). In this interim report, we demonstrate that a booster dose of ChAdOx1 nCoV-19 is safe and better tolerated than priming doses. Using a systems serology approach we also demonstrate that anti-spike neutralizing antibody titers, as well as Fc-mediated functional antibody responses, including antibody-dependent neutrophil/monocyte phagocytosis, complement activation and natural killer cell activation, are substantially enhanced by a booster dose of vaccine. A booster dose of vaccine induced stronger antibody responses than a dose-sparing half-dose boost, although the magnitude of T cell responses did not increase with either boost dose. These data support the two-dose vaccine regime that is now being evaluated in phase 3 clinical trials.
quote:Infectivity of asymptomatic versus symptomatic COVID-19
Negative binomial regression revealed that when adjusted for age, gender, and serology of index case, the incidence of COVID-19 among close contacts of a symptomatic index case was 3·85 times higher than for close contacts of an asymptomatic index case (95% CI2·06–7·19; p<0·0001; appendix).
Our findings suggest that people with asymptomatic COVID-19 are infectious but might be less infectious than symptomatic cases. We also identified that the proportion of close contacts who became infected did not depend on the serology status of the index case. One reason for this observation could be that close contacts tend to live or work with the index case and are exposed because of their regular contact with a person who was infectious before turning seropositive.
quote:High rate of persistent symptoms up to 4 months after community and hospital-managed SARS-CoV-2 infection
Recovery after severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection remains uncertain. A considerable proportion of patients experience persistent symptoms after SARS-CoV-2 infection which impacts health-related quality of life and physical function. Multi-disciplinary follow-up is recommended for patients with post-COVID illness and to assess health-related quality of life and physical function.
Over immuniteit en herinfectie. Onderzoek bij medewerkers in de zorg.quote:Antibody Status and Incidence of SARS-CoV-2 Infection in Health Care Workers
Background
The relationship between the presence of antibodies to severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and the risk of subsequent reinfection remains unclear.
Methods
We investigated the incidence of SARS-CoV-2 infection confirmed by polymerase chain reaction (PCR) in seropositive and seronegative health care workers attending testing of asymptomatic and symptomatic staff at Oxford University Hospitals in the United Kingdom. Baseline antibody status was determined by anti-spike (primary analysis) and anti-nucleocapsid IgG assays, and staff members were followed for up to 31 weeks. We estimated the relative incidence of PCR-positive test results and new symptomatic infection according to antibody status, adjusting for age, participant-reported gender, and changes in incidence over time.
Results
A total of 12,541 health care workers participated and had anti-spike IgG measured; 11,364 were followed up after negative antibody results and 1265 after positive results, including 88 in whom seroconversion occurred during follow-up. A total of 223 anti-spike–seronegative health care workers had a positive PCR test (1.09 per 10,000 days at risk), 100 during screening while they were asymptomatic and 123 while symptomatic, whereas 2 anti-spike–seropositive health care workers had a positive PCR test (0.13 per 10,000 days at risk), and both workers were asymptomatic when tested (adjusted incidence rate ratio, 0.11; 95% confidence interval, 0.03 to 0.44; P=0.002). There were no symptomatic infections in workers with anti-spike antibodies. Rate ratios were similar when the anti-nucleocapsid IgG assay was used alone or in combination with the anti-spike IgG assay to determine baseline status.
Conclusions
The presence of anti-spike or anti-nucleocapsid IgG antibodies was associated with a substantially reduced risk of SARS-CoV-2 reinfection in the ensuing 6 months. (Funded by the U.K. Government Department of Health and Social Care and others.)
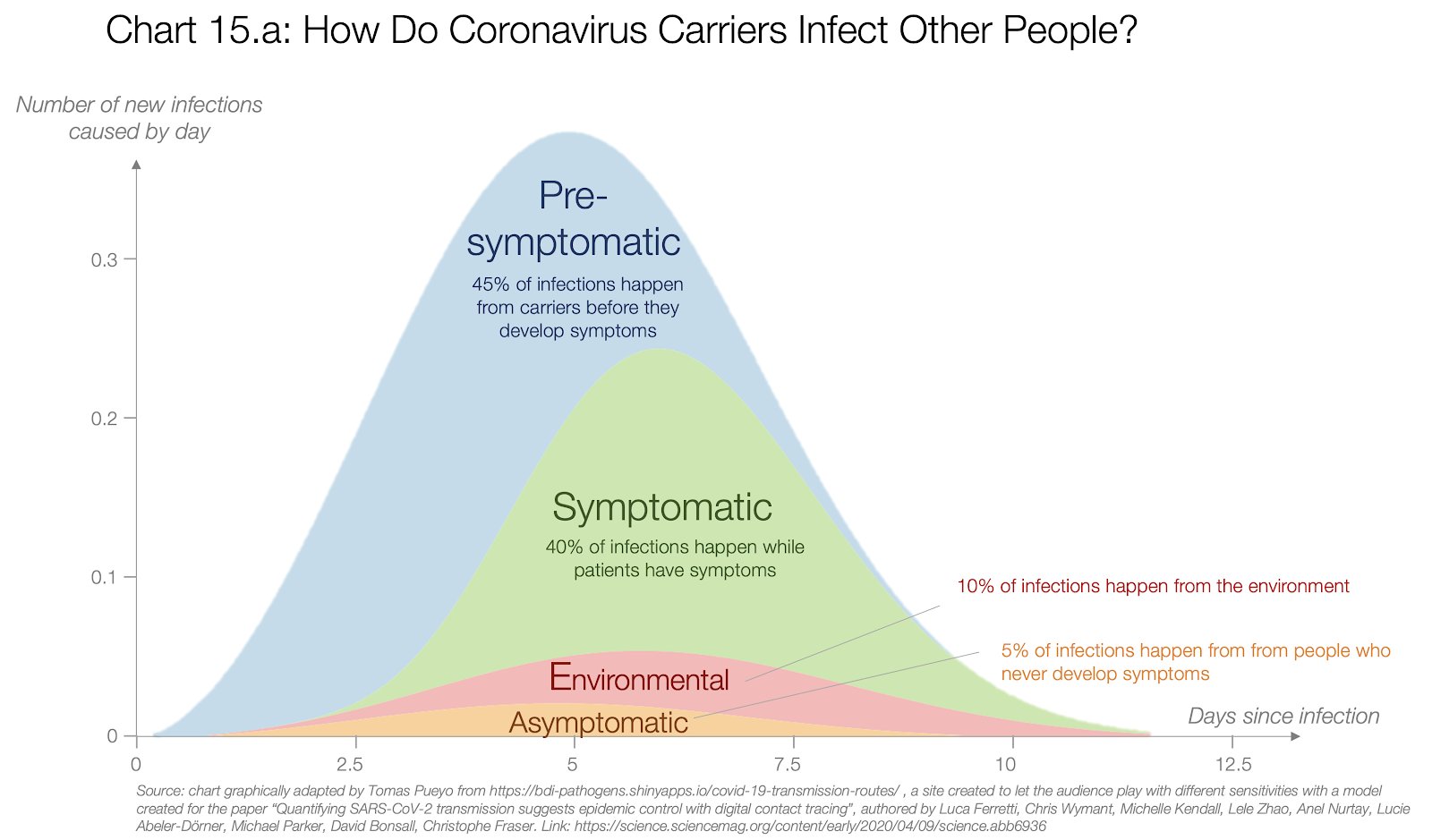
quote:Transmission of SARS-CoV-2 LineageB.1.1.7 in England: Insights from linkingepidemiological and genetic data
The SARS-CoV-2 lineage B.1.1.7, now designated Variant of Concern 202012/01 (VOC) byPublic Health England, originated in the UK in late Summer to early Autumn 2020. We examineepidemiological evidence for this VOC having a transmission advantage from severalperspectives. First, whole genome sequence data collected from community-based diagnostictesting provides an indication of changing prevalence of different genetic variants through time.Phylodynamic modelling additionally indicates that genetic diversity of this lineage has changedin a manner consistent with exponential growth. Second, we find that changes in VOCfrequency inferred from genetic data correspond closely to changes inferred by S-gene targetfailures (SGTF) in community-based diagnostic PCR testing. Third, we examine growth trends inSGTF and non-SGTF case numbers at local area level across England, and show that the VOC
has higher transmissibility than non-VOC lineages, even if the VOC has a different latent periodor generation time. Available SGTF data indicate a shift in the age composition of reportedcases, with a larger share of under 20 year olds among reported VOC than non-VOC cases.Fourth, we assess the association of VOC frequency with independent estimates of the overallSARS-CoV-2 reproduction number through time. Finally, we fit a semi-mechanistic modeldirectly to local VOC and non-VOC case incidence to estimate the reproduction numbers overtime for each. There is a consensus among all analyses that the VOC has a substantialtransmission advantage, with the estimated difference in reproduction numbers between VOCand non-VOC ranging between 0.4 and 0.7, and the ratio of reproduction numbers varyingbetween 1.4 and 1.8. We note that these estimates of transmission advantage apply to a periodwhere high levels of social distancing were in place in England; extrapolation to othertransmission contexts therefore requires caution
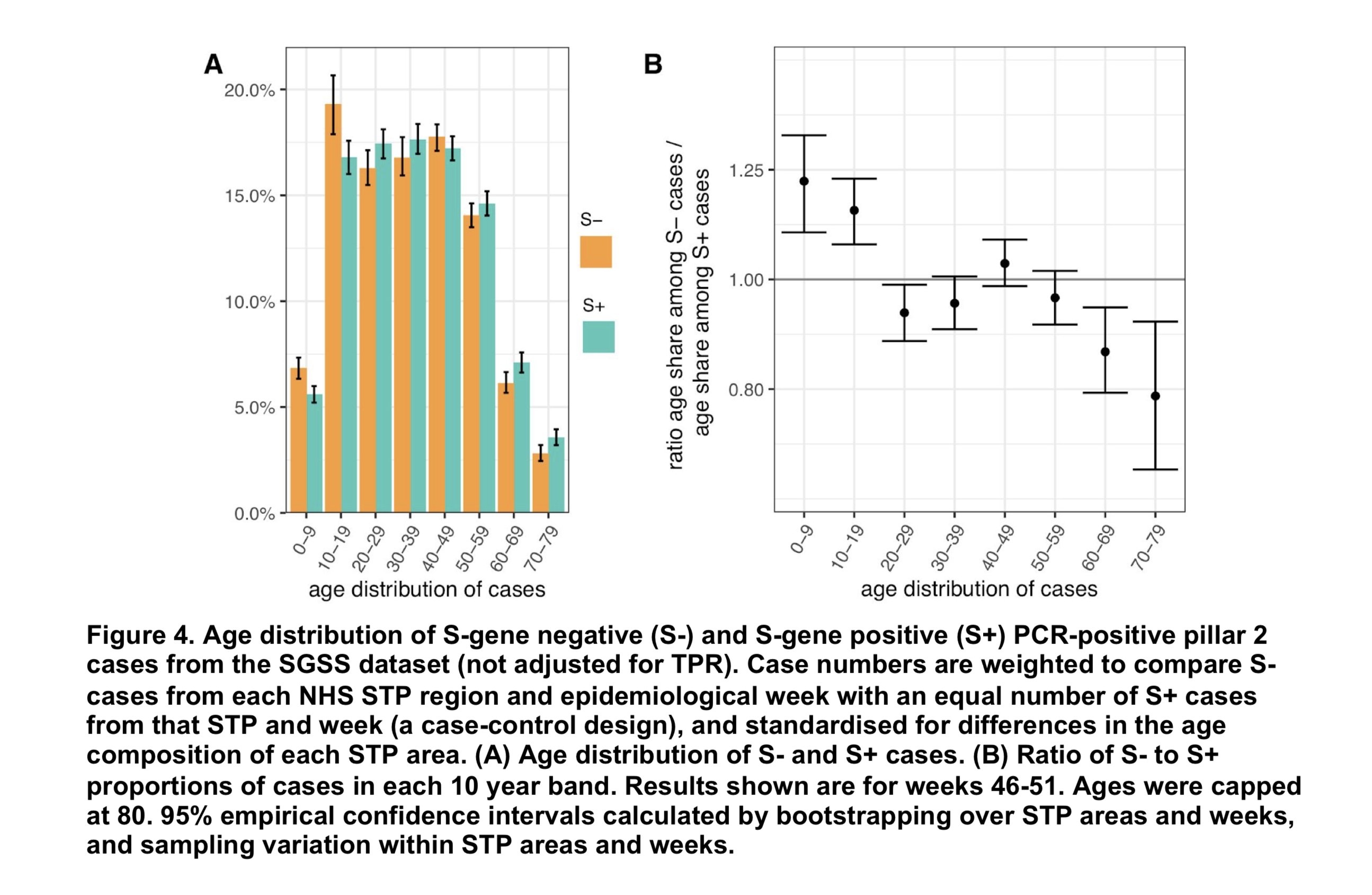
Interessant verband tussen comorbidity en viral load op de PCR testquote:Association between upper respiratory tract viral load, comorbidities, disease severity and outcome of patients with SARS-CoV-2 infection
Abstract
Background
There is limited information on the association between upper respiratory tract (URT) viral loads, host factors, and disease severity in SARS-CoV-2 infected patients.
Methods
We studied 1,122 patients (mean age: 46 years) diagnosed by PCR. URT viral load, measured by PCR cycle threshold, was categorized as high, moderate or low.
Results
There were 336 (29.9%) patients with comorbidities; 309 patients (27.5%) had high, 316 (28.2%) moderate, and 497 (44.3%) low viral load. In univariate analyses, compared to patients with moderate or low viral load, patients with high viral load were older, had more often comorbidities, developed symptomatic disease, were intubated and died; in addition, patients with high viral load had longer stay in intensive care unit and longer intubation compared to patients with low viral load (p-values <0.05 for all). Patients with chronic cardiovascular disease, hypertension, chronic pulmonary disease, immunosuppression, obesity and chronic neurological disease had more often high viral load (p-value<0.05 for all). Multivariate analysis found that a high viral load was associated with COVID-19. The level of viral load was not associated with any other outcome.
Conclusions
URT viral load could be used to identify patients at higher risk for morbidity or severe outcome.
Over "Long covid" patienten die langdurig klachten heeft.quote:6-month consequences of COVID-19 in patients discharged from hospital: a cohort study
Background
The long-term health consequences of COVID-19 remain largely unclear. The aim of this study was to describe the long-term health consequences of patients with COVID-19 who have been discharged from hospital and investigate the associated risk factors, in particular disease severity.
Methods
We did an ambidirectional cohort study of patients with confirmed COVID-19 who had been discharged from Jin Yin-tan Hospital (Wuhan, China) between Jan 7, 2020, and May 29, 2020. Patients who died before follow-up, patients for whom follow-up would be difficult because of psychotic disorders, dementia, or re-admission to hospital, those who were unable to move freely due to concomitant osteoarthropathy or immobile before or after discharge due to diseases such as stroke or pulmonary embolism, those who declined to participate, those who could not be contacted, and those living outside of Wuhan or in nursing or welfare homes were all excluded. All patients were interviewed with a series of questionnaires for evaluation of symptoms and health-related quality of life, underwent physical examinations and a 6-min walking test, and received blood tests. A stratified sampling procedure was used to sample patients according to their highest seven-category scale during their hospital stay as 3, 4, and 5–6, to receive pulmonary function test, high resolution CT of the chest, and ultrasonography. Enrolled patients who had participated in the Lopinavir Trial for Suppression of SARS-CoV-2 in China received severe acute respiratory syndrome coronavirus 2 antibody tests. Multivariable adjusted linear or logistic regression models were used to evaluate the association between disease severity and long-term health consequences.
Findings
In total, 1733 of 2469 discharged patients with COVID-19 were enrolled after 736 were excluded. Patients had a median age of 57·0 (IQR 47·0–65·0) years and 897 (52%) were men. The follow-up study was done from June 16, to Sept 3, 2020, and the median follow-up time after symptom onset was 186·0 (175·0–199·0) days. Fatigue or muscle weakness (63%, 1038 of 1655) and sleep difficulties (26%, 437 of 1655) were the most common symptoms. Anxiety or depression was reported among 23% (367 of 1617) of patients. The proportions of median 6-min walking distance less than the lower limit of the normal range were 24% for those at severity scale 3, 22% for severity scale 4, and 29% for severity scale 5–6. The corresponding proportions of patients with diffusion impairment were 22% for severity scale 3, 29% for scale 4, and 56% for scale 5–6, and median CT scores were 3·0 (IQR 2·0–5·0) for severity scale 3, 4·0 (3·0–5·0) for scale 4, and 5·0 (4·0–6·0) for scale 5–6. After multivariable adjustment, patients showed an odds ratio (OR) 1·61 (95% CI 0·80–3·25) for scale 4 versus scale 3 and 4·60 (1·85–11·48) for scale 5–6 versus scale 3 for diffusion impairment; OR 0·88 (0·66–1·17) for scale 4 versus scale 3 and OR 1·77 (1·05–2·97) for scale 5–6 versus scale 3 for anxiety or depression, and OR 0·74 (0·58–0·96) for scale 4 versus scale 3 and 2·69 (1·46–4·96) for scale 5–6 versus scale 3 for fatigue or muscle weakness. Of 94 patients with blood antibodies tested at follow-up, the seropositivity (96·2% vs 58·5%) and median titres (19·0 vs 10·0) of the neutralising antibodies were significantly lower compared with at the acute phase. 107 of 822 participants without acute kidney injury and with estimated glomerular filtration rate (eGFR) 90 mL/min per 1·73 m2 or more at acute phase had eGFR less than 90 mL/min per 1·73 m2 at follow-up.
Interpretation
At 6 months after acute infection, COVID-19 survivors were mainly troubled with fatigue or muscle weakness, sleep difficulties, and anxiety or depression. Patients who were more severely ill during their hospital stay had more severe impaired pulmonary diffusion capacities and abnormal chest imaging manifestations, and are the main target population for intervention of long-term recovery.
Over het effect van verplichte maatregelen in 10 landen waaronder Nederland.quote:Assessing Mandatory Stay‐at‐Home and Business Closure Effects on the Spread of COVID‐19
Background and Aims
The most restrictive non‐pharmaceutical interventions (NPIs) for controlling the spread of COVID‐19 are mandatory stay‐at‐home and business closures. Given the consequences of these policies, it is important to assess their effects. We evaluate the effects on epidemic case growth of more restrictive NPIs (mrNPIs), above and beyond those of less restrictive NPIs (lrNPIs).
Methods
We first estimate COVID‐19 case growth in relation to any NPI implementation in subnational regions of 10 countries: England, France, Germany, Iran, Italy, Netherlands, Spain, South Korea, Sweden, and the US. Using first‐difference models with fixed effects, we isolate the effects of mrNPIs by subtracting the combined effects of lrNPIs and epidemic dynamics from all NPIs. We use case growth in Sweden and South Korea, two countries that did not implement mandatory stay‐at‐home and business closures, as comparison countries for the other 8 countries (16 total comparisons).
Results
Implementing any NPIs was associated with significant reductions in case growth in 9 out of 10 study countries, including South Korea and Sweden that implemented only lrNPIs (Spain had a non‐significant effect). After subtracting the epidemic and lrNPI effects, we find no clear, significant beneficial effect of mrNPIs on case growth in any country. In France, e.g., the effect of mrNPIs was +7% (95CI ‐5%‐19%) when compared with Sweden, and +13% (‐12%‐38%) when compared with South Korea (positive means pro‐contagion). The 95% confidence intervals excluded 30% declines in all 16 comparisons and 15% declines in 11/16 comparisons.
Conclusions
While small benefits cannot be excluded, we do not find significant benefits on case growth of more restrictive NPIs. Similar reductions in case growth may be achievable with less restrictive interventions.
quote:
[..]
Over het effect van verplichte maatregelen in 10 landen waaronder Nederland.
Jammer dat Ioannidis door velen als niet (meer) salonfähig is verklaard door zijn "dwarse" denkbeelden en artikelen.
quote:Increased infections, but not viral burden, with a new SARS-CoV-2 variant
Background A new variant of SARS-CoV-2, B.1.1.7/VOC202012/01, was identified in the UK in December-2020. Direct estimates of its potential to enhance transmission are limited.
Methods Nose and throat swabs from 28-September-2020 to 2-January-2021 in the UK’s nationally representative surveillance study were tested by RT-PCR for three genes (N, S and ORF1ab). Those positive only on ORF1ab+N, S-gene target failures (SGTF), are compatible with B.1.1.7/VOC202012/01. We investigated cycle threshold (Ct) values (a proxy for viral load), percentage of positives, population positivity and growth rates in SGTF vs non-SGTF positives.
Results 15,166(0.98%) of 1,553,687 swabs were PCR-positive, 8,545(56%) with three genes detected and 3,531(23%) SGTF. SGTF comprised an increasing, and triple-gene positives a decreasing, percentage of infections from late-November in most UK regions/countries, e.g. from 15% to 38% to 81% over 1.5 months in London. SGTF Ct values correspondingly declined substantially to similar levels to triple-gene positives. Population-level SGTF positivity remained low (<0.25%) in all regions/countries until late-November, when marked increases with and without self-reported symptoms occurred in southern England (to 1.5-3%), despite stable rates of non-SGTF cases. SGTF positivity rates increased on average 6% more rapidly than rates of non-SGTF positives (95% CI 4-9%) supporting addition rather than replacement with B.1.1.7/VOC202012/01. Excess growth rates for SGTF vs non-SGTF positives were similar in those up to high school age (5% (1-8%)) and older individuals (6% (4-9%)).
Conclusions Direct population-representative estimates show that the B.1.1.7/VOC202012/01 SARS-CoV-2 variant leads to higher infection rates, but does not seem particularly adapted to any age group.
Epidemiology of post-COVID syndromefollowing hospitalisationwith coronavirus: a retrospective cohort study
Bijna 1/3 van patienten in Engeland ontslagen uit het ziekenhuis na Covid moesten binnen 5 maanden weer opgenomen worden, bijna 1/8ste overleed alsnog.
Bijna 1/3 van patienten in Engeland ontslagen uit het ziekenhuis na Covid moesten binnen 5 maanden weer opgenomen worden, bijna 1/8ste overleed alsnog.
quote:Individuals discharged from hospital following COVID-19 face elevated rates of multi-organdysfunction compared with background levels, and the increase in risk is neitherconfined to the elderly nor uniform across ethnicities.The diagnosis, treatment and preventionof PCSrequire integrated rather than organ-or disease-specific approaches. Urgent research is required to establish risk factors for PCS
Omdat we nu natuurlijk druk bezig zijn over de avondklok die eraan komt
Efficacy of Nationwide Curfew to Encounter Spread of COVID-19: A Case From Jordan
Efficacy of Nationwide Curfew to Encounter Spread of COVID-19: A Case From Jordan
quote:An Early Assessment of Curfew and SecondCOVID-19 Lock-down on Virus Propagationin France∗
This note provides an early assessment of the reinforced measures to curb the COVID-19pandemic in France, which include a curfew of selected areas and culminate in a second COVID-19-relatedlock-down that started on October 30, 2020 and is still ongoing. We analyse the change in virus propagationacross age groups and across départements using an acceleration index introduced in Baunez et al. (2020).We find that while the pandemic is still in the acceleration regime, acceleration decreased notably withcurfew measures and this more rapidly so for the more vulnerable population group, that is, for peopleolder than 60. Acceleration continued to decline under lock-down, but more so for the active populationunder 60 than for those above 60. For the youngest population aged 0 to 19, curfew measures did not reduce acceleration but lock-down does. This suggests that if health policies aim at protecting the elderly population generally more at risk to suffer severe consequences from COVID-19, curfew measures may be effective enough. However, looking at the departmental map of France, we find that curfews have notnecessarily been imposed in départements where acceleration was the largest.
quote:The Effect of Curfew Enforcement on Health Care Provision in COVID-19 Pandemic
The COVID-19 disease occurred in the final weeks of 2019. As part of the fight against COVID-19, countries have taken actions such as travel restrictions, suspension of border crossings and international flights, voluntary home isolation, public activities restriction, and curfews. The objective of this study is to identify the effect of curfew enforcement during the COVID-19 pandemic to determine and identify whether curfew has a positive effect on the health care workload. The number of patients admitted to Sakarya University Training and Research Hospital, their means of arrival, hospitalization-discharge, demographic characteristics were examined retrospectively for the period of curfew in April and May 2020 and the corresponding days in 2019. The significant statistical differences between the two periods were analyzed. The results of this research reveal that 24.488 patients were admitted to our emergency department. Of these patients, 12813 (52.3%) were male, 11675 (47.7%) were female. The number of emergency department admissions of the pediatric age group decreased from 1822 (8.9%) to 33 patients (0.8%). Moreover, the number of patients admitted to the emergency service in the related period of 2019 was 20548 (83.9%), while this figure decreased to 3940 individuals (16.1%) during the curfew period. It was implied that curfew could reduce the unnecessary admissions to hospitals, the number of ambulance usage, and provide a positive contribution to the reduction in traumas, car accidents, work accidents, and forensic cases during pandemic.
Evolution of antibody immunity to SARS-CoV-2
Besproken door Derek Lowe in zijn science blog hier.quote:Abstract
Severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) has infected 78 million individuals and is responsible for over 1.7 million deaths to date. Infection is associated with development of variable levels of antibodies with neutralizing activity that can protect against infection in animal models1,2. Antibody levels decrease with time, but the nature and quality of the memory B cells that would be called upon to produce antibodies upon re-infection has not been examined. Here we report on the humoral memory response in a cohort of 87 individuals assessed at 1.3 and 6.2 months after infection. We find that IgM, and IgG anti-SARS-CoV-2 spike protein receptor binding domain (RBD) antibody titres decrease significantly with IgA being less affected. Concurrently, neutralizing activity in plasma decreases by fivefold in pseudotype virus assays. In contrast, the number of RBD-specific memory B cells is unchanged. Memory B cells display clonal turnover after 6.2 months, and the antibodies they express have greater somatic hypermutation, increased potency and resistance to RBD mutations, indicative of continued evolution of the humoral response. Analysis of intestinal biopsies obtained from asymptomatic individuals 4 months after the onset of coronavirus disease-2019 (COVID-19), using immunofluorescence, or polymerase chain reaction, revealed persistence of SARS-CoV-2 nucleic acids and immunoreactivity in the small bowel of 7 out of 14 volunteers. We conclude that the memory B cell response to SARS-CoV-2 evolves between 1.3 and 6.2 months after infection in a manner that is consistent with antigen persistence.
Identifying COVID-19 Risk Through Observational Studies to Inform Control Measures
A year into the coronavirus disease 2019 (COVID-19) pandemic there remains an urgent need to limit severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) spread and to curb the pandemic in the US through nonpharmaceutical interventions. Clear evidence supports the effectiveness of simple strategies in identifying risks and mitigating the spread of infection, with much of this evidence coming from observational studies. Community risk factors for infection can be identified by comparing recent behaviors and exposures among people who have been infected with those who are not infected using a traditional case-control approach. High-risk environments identified from these investigations need to be clearly communicated to the public to support public health measures and motivate individual behavior change to reduce the risk of infection.
A year into the coronavirus disease 2019 (COVID-19) pandemic there remains an urgent need to limit severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) spread and to curb the pandemic in the US through nonpharmaceutical interventions. Clear evidence supports the effectiveness of simple strategies in identifying risks and mitigating the spread of infection, with much of this evidence coming from observational studies. Community risk factors for infection can be identified by comparing recent behaviors and exposures among people who have been infected with those who are not infected using a traditional case-control approach. High-risk environments identified from these investigations need to be clearly communicated to the public to support public health measures and motivate individual behavior change to reduce the risk of infection.

Op basis daarvan zou je kunnen zeggen dat de kans op besmetting eigenlijk alleen in restaurants echt hoger is, en mogelijk ook in cafes. OR = odds ratio
Winkelen, salons, thuisbezoek, public transport heeft allemaal niet of nauwelijks invloed. Mogelijk is er een verhoogde kans in gyms en kerken, maar dat is niet overtuigend.
Winkelen, salons, thuisbezoek, public transport heeft allemaal niet of nauwelijks invloed. Mogelijk is er een verhoogde kans in gyms en kerken, maar dat is niet overtuigend.
volgens mij kun je dat nog lang niet uit dat onderzoek halen...quote:
Op basis daarvan zou je kunnen zeggen dat de kans op besmetting eigenlijk alleen in restaurants echt hoger is, en mogelijk ook in cafes. OR = odds ratio
Winkelen, salons, thuisbezoek, public transport heeft allemaal niet of nauwelijks invloed. Mogelijk is er een verhoogde kans in gyms en kerken, maar dat is niet overtuigend.
het betreft een specifiek naar beweegpatronen, waarbij men het beweegpatroon en activiteiten van personen die covid-positief waren vastgelegd heeft (359 personen uit 10 verschillende staten, telefonisch ondervraagt, daarnaast ook een controlegroep van 160 personen, die niet covid-positief waren )
de eerste groep van 154 personen had aangegeven een directe contactpersoon te hebben die al eerder als covid-positief gemeld was (en dus een mogelijke bron van de besmetting was)
en een andere groep van 205 personen kon niet aangeven of ze een andere contactpersoon hadden die als mogelijke bron kon gelden.
Ze vergelijken nu het beweegpatroon van de besmette mensen met de controlegroep van niet besmette, waarbij er onderscheid gemaakt wordt tussen mensn die een direkte contactpersoon hadden die ook besmet was of die dat niet konden aangeven.
Het enige wat mij heel duidelijk opvalt is de ontzettend hoge score van mensen die geen bekend covid-positieve contactpersoon hebben, maar wel zelfs positief getest zijn, en die kennelijk zeer regelmatig nog een bar bezocht hebben.
(de band loopt overigens verder naar rechts en valt buiten de grafiek tot een maximale breedte van boven de 10, de afbeelding was niet breed genoeg om dat weer te geven).
verder lijken overall besmette personen vaker cafe's, restaurants, fitness studios en/of kerken te bezoeken dan de controlegroep, maar dat bewijst an sich nog niet dat dat de plek is waar ze besmet zijn...
hooguit wijst hun beweegpatroon wel op dat ze sociaal actiever zijn dan anderen.
Dat bv zaken als winkelen of gebruik van OV, en het hebben van thuisbezoek niet opvallend er uitsteekt, kan goed komen doordat het ook geen substantiele verschillen zijn tussen mensn die wél bemet raken en die die dat niet doen... wat echter ok niet veel bewijst over het risico, hooguit dat weinig mensen er geheel mee kunnen of willen ophouden, het vavak gewoon essentiele activiteiten zijn die iedereen moet doen
"Whatever you feel like: Life’s not one color, nor are you my only reader" - Ausonius, Epigrammata 25
Thanks voor de correctie, ik was duidelijk nog niet wakker! Ga het nog eens goed lezen dan.quote:
[..]
volgens mij kun je dat nog lang niet uit dat onderzoek halen...
het betreft een specifiek naar beweegpatronen, waarbij men het beweegpatroon en activiteiten van personen die covid-positief waren vastgelegd heeft (359 personen uit 10 verschillende staten, telefonisch ondervraagt, daarnaast ook een controlegroep van 160 personen, die niet covid-positief waren )
de eerste groep van 154 personen had aangegeven een directe contactpersoon te hebben die al eerder als covid-positief gemeld was (en dus een mogelijke bron van de besmetting was)
en een andere groep van 205 personen kon niet aangeven of ze een andere contactpersoon hadden die als mogelijke bron kon gelden.
Ze vergelijken nu het beweegpatroon van de besmette mensen met de controlegroep van niet besmette, waarbij er onderscheid gemaakt wordt tussen mensn die een direkte contactpersoon hadden die ook besmet was of die dat niet konden aangeven.
Het enige wat mij heel duidelijk opvalt is de ontzettend hoge score van mensen die geen bekend covid-positieve contactpersoon hebben, maar wel zelfs positief getest zijn, en die kennelijk zeer regelmatig nog een bar bezocht hebben.
(de band loopt overigens verder naar rechts en valt buiten de grafiek tot een maximale breedte van boven de 10, de afbeelding was niet breed genoeg om dat weer te geven).
verder lijken overall besmette personen vaker cafe's, restaurants, fitness studios en/of kerken te bezoeken dan de controlegroep, maar dat bewijst an sich nog niet dat dat de plek is waar ze besmet zijn...
hooguit wijst hun beweegpatroon wel op dat ze sociaal actiever zijn dan anderen.
Dat bv zaken als winkelen of gebruik van OV, en het hebben van thuisbezoek niet opvallend er uitsteekt, kan goed komen doordat het ook geen substantiele verschillen zijn tussen mensn die wél bemet raken en die die dat niet doen... wat echter ok niet veel bewijst over het risico, hooguit dat weinig mensen er geheel mee kunnen of willen ophouden, het vavak gewoon essentiele activiteiten zijn die iedereen moet doen
via twitter om gelijk een samevatting te hebben:
https://twitter.com/Roxytonin/status/1372801396039249923
https://twitter.com/Roxytonin/status/1372801396039249923
Is dat figuur in een resolutie uit het jaar 0 geupload of laadt mijn laptop het niet?quote:
via twitter om gelijk een samevatting te hebben:
https://twitter.com/Roxytonin/status/1372801396039249923
Ze hebben ook een blog erover geschreven: https://blogs.bmj.com/bmj/2021/03/19/a-birds-eye-view-of-the-risk-of-covid-19-infection-from-children/
|
|
| Forum Opties | |
|---|---|
| Forumhop: | |
| Hop naar: | |