COR Corona COVID-19 forum
Alles over het corona / COVID-19 virus.



![1R1BRNu.png]afbeelding](https://i.imgur.com/1R1BRNu.png]afbeelding)
Houd minimaal 1.5 meter afstand met anderen buiten je huishouden in alle gevallen.
Vragen over je eigen gezondheid: huisarts of GGD
Andere vragen: 0800-1351 (08:00-22:00)
Helpen?
https://www.makers4all.eu/nl/
https://www.extrahandenvoordezorg.nl/
https://www.rodekruis.nl/hulp-in-nederland/ready2help/
Informatie & achtergronden:
• Wikipedia
• Dr. John Campbell met een dagelijkse update
• Dit doet corona met je, als je pech hebt.
• Simulaties over waarom social distancing werkt
• Video: Wat is exponentiële groei en hoe werkt dat bij uitbraken
• Video: Wat is dit coronavirus, wat doet het, wat zijn de maatregelen
• Alle artikelen over Covid zijn gratis te lezen op de financial times
• Wetenschappelijk Covid19 HUB voor publicaties (dus voor wetenschappelijk geinteresseerden)
• Universiteitsindex Leiden
Nederland:
• RIVM Rijksinstituut voor Volksgezondheid en Milieu - actuele informatie
• Besmettingen per gemeente (RIVM-kaartje)
• arcgis kaart van NL
• Corona-patiënten op de Nederlanders IC's
• Reconstructie NRC, een echte aanrader
Internationale organisaties:
• ECDC European Centre for Disease Prevention and Control
• WHO World Health Organisation
Aantallen & Trackers:
• Overzicht JHU
• Overzicht Worldometers
• Overzicht thebaselab
• Overzicht WHO
• Overzicht BNO News
• Alle gevallen, in een lijst
• Grafieken zelf maken of Alle grafieken t/m 13apr20
• Spreadsheet met cijfers die user joyvke tot 15apr20 bijhield
• Netherlands & Italy compare infected CORONAvirus (COVID-19) infected daily graph/chart
• Verzameling alle NL cijfers
Timelapse:
• Flourish
COVID-19 feiten
• vooral hoest- en niesdruppeltjes zorgen voor overdracht
• de besmetting is meer dan bij seizoensgriep, maar gelukkig minder dan bij mazelen (2 < R0 < 3)
• verreweg de meesten hebben lichte (griepachtige) klachten
• bijna alle sterfgevallen betreffen ouderen of al zieke mensen
Bron
Gedragsregels in dit topic:
• Probeer niet lollig te doen
• Bij nieuws: graag een bron
• Geen opruiende berichten
• Volg de aanwijzingen van de moderatie op
• Ga niet off-topic
• Geen slowchat in dit topic. Hier is het slowchat-topic: COR / [En Don SC #1] HATSJOE
• Let een beetje op elkaar
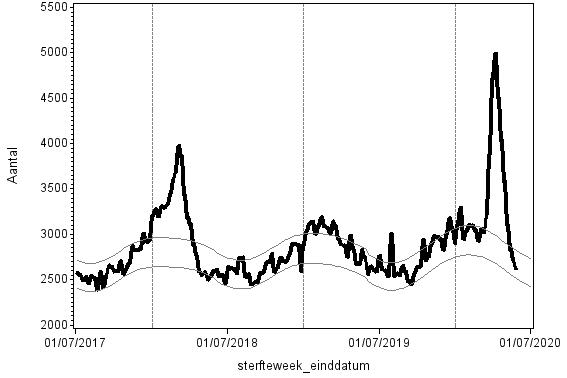
Oversterfte met als oorzaak griep (2018) en Covid-19 (2020)
Vermijd drukte!

Moderatie:
@trein2000 @capricia @onlogisch @Lonaa @Muck @Lavenderr @Kyran @Sounddragon @D_A
Vaag gezever over deugpartijen?quote:Op maandag 13 juli 2020 12:25 schreef Monolith het volgende:
[..]
Ik heb geen idee waarop je dat baseert anders dan wat vaag gezever over 'deugpartijen'.
Komop, Christenunie en D66 zien vuur branden als ze FvD horen. Dat snap je zelf ook, die gaan nóóit samenwerken met FvD.
Je hoeft jezelf niet dom voor te doen je snapt best wel welke partijen ik bedoel.
Afgezien daarvan: Je hebt gelijk joh, CDA en VVD zijn net zo hard het zooitje aan het verneuken, echter, de vraag of het type beleid anders zou zijn met een FvD in dat rijtje, denk ik wel iets rechtser dan huidig ja.
"Het enkele feit dat de gewasbeschermingsmiddelen zijn toegelaten, geeft in ieder geval geen garantie op het ontbreken van met name een uitgesteld schadelijk effect op de gezondheid van mensen."

Gisteren ook een uitgebreid stuk in het Parool over de situatie in het toeristengebied van Amsterdam - 'alsof Corona niet meer bestaat'. De menselijke domheid kent geen grenzen, en daarnaast moeten de burgemeesters zich maar eens opnieuw achter de oren krabben waarom er zo weinig en zo slecht wordt gehandhaafd op de regels.quote:maandag 13 juli 2020 12:20 schreef Momo het volgende:twitter:martindrent twitterde op zondag 12-07-2020 om 20:36:38 Sommige kroegen in Groningen waren afgelopen weekend tjokvol. Bezoekers kunnen geen afstand houden, zeker niet met een drankje op. Lees meer, met reacties van de burgemeester @:gem_groningen en de horeca ➡️ https://t.co/IKxF9nIA7N Gemaakt met @:Sander_Slager #rtvnoord https://t.co/u4u77eXXCz reageer retweet
 Sommige kroegen in Groningen waren afgelopen weekend tjokvol. Bezoekers kunnen geen afstand houden, zeker niet met een drankje op. Lees meer, met reacties van de burgemeester @:gem_groningen en de horeca ➡️
Sommige kroegen in Groningen waren afgelopen weekend tjokvol. Bezoekers kunnen geen afstand houden, zeker niet met een drankje op. Lees meer, met reacties van de burgemeester @:gem_groningen en de horeca ➡️
Brutalen hebben de halve wereld; doe mij die andere helft dan maar


Dat bedoel ik natuurlijk niet. Ik bedoel je loze aantijgingen omtrent de opstelling van D66 en de CU omtrent coronamaatregelen.quote:
[..]
Vaag gezever over deugpartijen?
Komop, Christenunie en D66 zien vuur branden als ze FvD horen. Dat snap je zelf ook, die gaan nóóit samenwerken met FvD.
Je hoeft jezelf niet dom voor te doen je snapt best wel welke partijen ik bedoel.
Kijk, onder normale omstandigheden zou ik een kabinet PVV / FvD van harte toejuichen, omdat ik me echt kostelijk zou gaan amuseren om de complete clusterfuck die dat zou op gaan leveren. De LPF was al zo'n pareltje en ook Bolsonaro en Trump zijn best leuk, al zorgen die voor nogal wat leed in eigen land, maar goed daar woon ik niet. Onder deze omstandigheden zie ik echter liever gewoon capabele bestuurders.
Volkorenbrood: "Geen quotes meer in jullie sigs gaarne."
Kan die discussie over politieke partijen misschien elders?
“Rather than love, than money, than fame, give me truth.”
Ja er nog niets in de pers over, maar het lijkt op een clustertje in Rotterdam e.o. (~45 cases afgelopen weekend)
wegmetdetestwet.nl / wegmetdetestmaatschappij.nl voor een gratis subdomain DM me.
Ik zie het beleid van het kabinet, daar maken zij onderdeel van uit, en zie ze weinig weerstand bieden tegen het huidige beleid, ik heb echt helemaal 0.0 reden om aan te nemen dat zij er anders in zouden staan.quote:
Dat bedoel ik natuurlijk niet. Ik bedoel je loze aantijgingen omtrent de opstelling van D66 en de CU omtrent coronamaatregelen.
"Het enkele feit dat de gewasbeschermingsmiddelen zijn toegelaten, geeft in ieder geval geen garantie op het ontbreken van met name een uitgesteld schadelijk effect op de gezondheid van mensen."
Dat was het punt ook niet. Je stelt feitelijk eerst dat het huidige beleid in weerwil zou zijn van wat CDA en VVD zouden willen, maar onder druk van CU en D66 tot stand zou komen. Dat is wat anders dan zeggen dat D66 en CU geen bezwaar maken tegen het huidige beleid.quote:
[..]
Ik zie het beleid van het kabinet, daar maken zij onderdeel van uit, en zie ze weinig weerstand bieden tegen het huidige beleid, ik heb echt helemaal 0.0 reden om aan te nemen dat zij er anders in zouden staan.
Het huidige beleid is in mijn ogen vrij technocratisch met wel een vleugje VVD. Nederland is namelijk helemaal niet zo hard dichtgegaan. Na Zweden kende Nederland zo ongeveer de minst restrictieve maatregelen en inmiddels zijn de maatregelen in Zweden geloof ik alweer strikter dan hier. Ik zie niet in waarom CDA en VVD ook maar ergens iets zouden wijzigen qua koers als het FvD in het kabinet zou zitten.
Volkorenbrood: "Geen quotes meer in jullie sigs gaarne."
Hoe dan? Die partijen staan lijnrecht tegenover elkaar op het gebied van migratie, de EU en het klimaatbeleid. Ook hebben die drie bij lange na geen meerderheid in de eerste kamer.quote:
[..]
PVV zie ik dermate verketterd worden dat al halen ze 65 zetels, dat alleen FvD zijn vingers aan zou branden om daar een kabinet mee te vormen.
FvD zou toch moeten kunnen met CDA en VVD. Deugdrampartijen weggelaten.
Het volgende kabinet wordt gewoon weer een middenkabinet.
Geen politiek gelul over politieke partijen hier aub.
wegmetdetestwet.nl / wegmetdetestmaatschappij.nl voor een gratis subdomain DM me.
Omdat je met andere belangen te dealen hebt die een andere richting op wijzen.quote:
Ik zie niet in waarom CDA en VVD ook maar ergens iets zouden wijzigen qua koers als het FvD in het kabinet zou zitten.
"Het enkele feit dat de gewasbeschermingsmiddelen zijn toegelaten, geeft in ieder geval geen garantie op het ontbreken van met name een uitgesteld schadelijk effect op de gezondheid van mensen."
Ik zie niet in waarom de vraag wat de impact van verschillende politieke partijen op het beleid omtrent corona niet in deze reeks zou horen.
Volkorenbrood: "Geen quotes meer in jullie sigs gaarne."
Welke belangen zijn dat en welke richting wijzen ze op?quote:
[..]
Omdat je met andere belangen te dealen hebt die een andere richting op wijzen.
Volkorenbrood: "Geen quotes meer in jullie sigs gaarne."
Verschrikkelijk eigenlijk dat immigratieskeptisch pas bij FvD zou beginnen in dat geval.quote:
[..]
Hoe dan? Die partijen staan lijnrecht tegenover elkaar op het gebied van migratie, de EU en het klimaatbeleid. Ook hebben die drie bij lange na geen meerderheid in de eerste kamer.
Het volgende kabinet wordt gewoon weer een middenkabinet.
Maar ik denk dat je ongelijk hebt joh, zeker qua achterban zijn ze bij de VVD ook wel klaar met de immigratie en misschien ook wel bij het CDA.
"Het enkele feit dat de gewasbeschermingsmiddelen zijn toegelaten, geeft in ieder geval geen garantie op het ontbreken van met name een uitgesteld schadelijk effect op de gezondheid van mensen."
Kijk naar wat FvD wilt en u vindt uw antwoord.quote:
[..]
Welke belangen zijn dat en welke richting wijzen ze op?
"Het enkele feit dat de gewasbeschermingsmiddelen zijn toegelaten, geeft in ieder geval geen garantie op het ontbreken van met name een uitgesteld schadelijk effect op de gezondheid van mensen."
Leuk dat je dit denkt maar dit blijkt nergens uit. Gevalletje wishful thinking!quote:
[..]
Verschrikkelijk eigenlijk dat immigratieskeptisch pas bij FvD zou beginnen in dat geval.
Maar ik denk dat je ongelijk hebt joh, zeker qua achterban zijn ze bij de VVD ook wel klaar met de immigratie en misschien ook wel bij het CDA.
Hopelijk doen ze ook hun best om het lokaal de kop in te drukken als het zo is.quote:
Ja er nog niets in de pers over, maar het lijkt op een clustertje in Rotterdam e.o. (~45 cases afgelopen weekend)
Who knows! Christenunie en D66 zijn in ieder geval een stuk concreter in dat ze het allemaal leuk vinden! Dus ik heb hoop dat het er minder in zit bij CDA/VVD !quote:
[..]
Leuk dat je dit denkt maar dit blijkt nergens uit. Gevalletje wishful thinking!
"Het enkele feit dat de gewasbeschermingsmiddelen zijn toegelaten, geeft in ieder geval geen garantie op het ontbreken van met name een uitgesteld schadelijk effect op de gezondheid van mensen."

twitter:Newsweek twitterde op maandag 13-07-2020 om 12:00:16 Scans reveal heart damage in over half of COVID-19 patients in study https://t.co/EYyjOSkemd reageer retweet
 Scans reveal heart damage in over half of COVID-19 patients in study
Scans reveal heart damage in over half of COVID-19 patients in study
quote:Op maandag 13 juli 2020 12:53 schreef Momo het volgende:
twitter:Newsweek twitterde op maandag 13-07-2020 om 12:00:16 Scans reveal heart damage in over half of COVID-19 patients in study https://t.co/EYyjOSkemd reageer retweet
Lekker suggestieve titel weer.quote:On average, the participants were aged 62, and 70 percent were male. Sixty percent of the scans were performed in a critical care setting, such as an ICU unit or emergency room, while the others were carried out in general medicine settings, cardiology, respiratory, or COVID-19 wards. Some 54 percent of the patients had severe COVID-19.
blablablabla
Inmiddels zou ik toch wel eens een overzicht willen zien van het aantal mensen die langdurige of blijvende schade door Covid oplopen. Ik lees van alles over mensen die maar niet beter worden, chronisch moe blijven, blijvende longschade, hartklachten of schade aan andere organen oplopen. Maar hoeveel zijn het er nu precies? Lijkt me toch ook wel van belang in het beleid. Zeker als we niet lang immuun blijven.quote:twitter:Newsweek twitterde op maandag 13-07-2020 om 12:00:16 Scans reveal heart damage in over half of COVID-19 patients in study https://t.co/EYyjOSkemd reageer retweet
Je kunt ook beter gelijk doorklikken naar de wetenschappelijke publicatie en dan de discussiesectie lezen:quote:
quote:We report findings from the first international survey of echocardiography in patients with confirmed or suspected COVID-19. Data from 1216 patients scanned in 69 countries across six continents demonstrated left or right ventricular abnormalities in half of all patients with COVID-19 undergoing echocardiography, and that these abnormalities were severe in 1 in 7 patients. The majority had non-specific patterns of ventricular dysfunction, although new myocardial infarction, myocarditis, and takotsubo cardiomyopathy were observed in a minority of patients. Echocardiography was reported to directly change patient management in a third of cases including alterations to disease-specific management, haemodynamic support, and the level of care received by the patients.
The simple online format of this survey allowed rapid capture of the echocardiographic findings from a large number of patients with COVID-19 during the pandemic’s peak. This was facilitated by our ability to disseminate and to publicize the survey via social media and through an established global network of imaging specialists. This format allowed us to keep pace with the rapid spread of COVID-19 around the world. Most scans were performed in the current epicentres of the outbreak: the UK, Italy, Spain, France, and the USA. While undoubtedly a global survey, our data remain representative of the current geographical distribution of the virus.
Whilst our previous understanding of how COVID-19 affects the heart was limited to case reports and case series,7–9 consistent epidemiological data have demonstrated that patients with established cardiovascular disease, risk factors, or elevated cardiac biomarkers have an increased susceptibility to infection and an increased risk of severe disease and death.3–6 Severe cardiac disease was observed in 1 in 7 patients across the whole cohort and in 1 in 8 patients without pre-existing cardiac disease. This proportion rose to 1 in 5 when the indication for imaging included raised cardiac biomarkers. The proportion of abnormal echocardiograms and those demonstrating severe cardiac disease were similar after excluding patients with previously established cardiac disease (heart failure, valve disease, or ischaemic heart disease), suggesting that in this population the cardiac abnormalities relate to COVID-19 infection.
The pattern of cardiac injury observed in our survey appears to be consistent with the cardiovascular involvement observed in patients with other severe viral respiratory infections.16–19 Right ventricular abnormalities were observed in a quarter of patients and were more common in patients with more severe symptoms of COVID-19. These are likely to reflect severe respiratory disease, including the viral pneumonia itself, as well as both clinical and subclinical pulmonary thrombo-embolism.20 Left ventricular abnormalities were present in a third of patients and were predominantly non-specific in nature. Further research is required to define the mechanism of this dysfunction as only occasionally were echocardiographic patterns consistent with myocardial infarction, myocarditis, or takotsubo cardiomyopathy. The latter conditions are often difficult to recognize during an isolated echocardiogram, particularly when performed in a critical care setting, and, as such, their true prevalence may have been underestimated.
In a third of patients who underwent echocardiography on clinical indication, imaging was reported to result in an immediate change in patient management. This included changes in disease-specific therapies, such as pericardiocentesis or therapy for heart failure, pulmonary embolism, or acute coronary syndromes. It also contributed to decisions regarding the level of patient care, such as the admission of patients to critical care, and the need for titration of haemodynamic support. In practice, this proportion may have been underestimated as echocardiographers may not have fully appreciated the consequences of their scan at the time of imaging. In addition, a majority of patients had echocardiography performed in an intensive care unit. In this setting, optimization of management may have been previously instituted or changes in management limited by severe respiratory or haemodynamic compromise. Few previous studies have reported the impact of echocardiography on changes in management, and none has been performed in a critical care setting.21 To put our findings into context, Bethge et al. report in an outpatient setting that whilst 22% of patients had abnormal findings, management changed in only 3% of patients.22 Finally, we suggest that information supporting the continuation of a management strategy may be as clinically relevant as information that leads to the initiation of an alternative strategy.
The complex logistics involved in performing echocardiography in patients with COVID-19 and the risk of virus transmission necessitates robust selection of patients for imaging.23 Our data do not imply that all patients with COVID-19 require an echocardiogram. Indeed, patients undergoing echocardiography here had clearly defined clinical indications. Our data suggest that cardiac biomarkers may help improve the selection of patients for imaging, with elevated BNP and cardiac troponin concentrations independent predictors of left and right ventricular abnormalities, respectively. Building on this study, there is now a need for future imaging and biomarker studies to systematically investigate the cardiovascular manifestations of COVID-19, and to establish their true prevalence. The CAPACITY-COVID European Registry aims to determine the role of cardiovascular disease in the COVID-19 pandemic through standardized large-scale data collection.24 Imaging with echocardiography and cardiovascular magnetic resonance following recovery from COVID-19 will be more readily achievable and will be well placed to define any residual cardiac damage caused by the condition. Similarly, studies investigating whether cardiac biomarkers can better direct clinical imaging and improve patient outcomes would be welcome.
Our study suffers from the usual limitations associated with an observational survey. Whilst by design we sought to conduct a rapid survey capturing key echocardiographic findings during the pandemic’s peak, this limited the amount and granularity of the data we could capture. We are reliant on operator-reported findings, as is common in clinical practice, and acknowledge that definitive assessment and core lab verification of cardiac function with echocardiography in critically ill patients is challenging. A proportion of the data was collected from free text-fields, and as such may be biased and represent an underestimate of these findings or clinical variables. Additionally, this survey is subject to substantial case selection bias. For example, we do not know the prevalence of abnormalities in those who did not undergo scanning. In view of the complex logistics around scanning, echocardiography was probably limited to those with clear clinical indications or those with increased disease severity. Furthermore, the use of echocardiography has probably decreased in the current pandemic due to concerns over viral transmission, and this may further contribute to the selection of patients for scanning. We did not capture patient outcomes, but many of the relevant outcomes have yet to occur. Finally, there were relatively few data from certain countries, including China. As the survey continues, we will seek to better target and gather more information from these countries, with further reports to follow.
In this global survey, cardiac abnormalities were observed in half of all COVID-19 patients undergoing echocardiography. Abnormalities were often unheralded or severe, and imaging changed management in one-third of patients.
Volkorenbrood: "Geen quotes meer in jullie sigs gaarne."