BNW Brave New World
Samenzwering, verborgen agenda's en geheime geschiedenis. De zoektocht naar de wereld die achter de façade van alledag ligt.



quote:Op donderdag 18 april 2013 19:29 schreef Terecht het volgende:
[..]
Ik snap niets van je reactie, sorry. Wat bedoel je hiermee?
Nee, over mensen als Alex Jones en David Icke. Ze bedoelen het zelf goed, alleen ze zijn gewoon puppets van de elite. Mensen die iets beginnen te begrijpen van de wereld gaan op onderzoek uit, komen vervolgens bij Alex of David uit omdat ze door de elite op het internet gepromoot worden, en krijgen zo de verkeerde info, de info die al lang door de filters van de elite zijn geweest. Hier gaat het dan ook fout, want die mensen die naar hen luisteren denken dat ze echt ''awake'' zijn, maar ze worden juist nog een keer gehersenspoeld. Ga vooral zelf op onderzoek uit en wees ruimdenkend, denk voor jezelf.quote:
Dus geloven dat er geen massamoord is gepleegd geeft blijkt van meer werkelijkheidszin dan geloven dat er een massamoord is gepleegd. Wat zou Orwell daarvan vinden?quote:
[..]
Ik WIL geloven niks.Als ik WIL wat geloven dan zou ik heel graag geloven dat alle mensen zijn lief en aardig en ze zullen nooit zoiets doen.
The crowning attainment of historical study is a historical sense - an intuitive understanding of how things do not happen. - Lewis Namier


ja maar dit gaat over de VS moet je na gaan hoe het geregeld in Afrika er aan toe gaat.quote:
[..]
Dus geloven dat er geen massamoord is gepleegd geeft blijkt van meer werkelijkheidszin dan geloven dat er een massamoord is gepleegd. Wat zou Orwell daarvan vinden?
hier hebben ze het over 3000 mensen waar geneens alle info klopt! in enschede vielen 23 slachtoffers en ze denken nog veel meer.
en dan bijvb naar Rwanda daar hebben ze alleen maar de schatting tussen de 500.000 en 1.000.000 slachtoffers.
ze weten het geeneens.
I am the hope of the universe. I am the answer to all living things that cry out for help.I am the protector of the innocent. I am the Light in the darkness. I am truth. Ally to good! Nightmare to you!
Aliens.quote:
Iemand een verklaring voor de spaghetti op deze brandweer auto?
[ afbeelding ]
Ik geloof in iets wanneer ik heb me genoeg over gelezen - dan heb ik 'n mening.quote:
[..]
Dus geloven dat er geen massamoord is gepleegd geeft blijkt van meer werkelijkheidszin dan geloven dat er een massamoord is gepleegd. Wat zou Orwell daarvan vinden?
IMO - is er genoeg bewijs dat die toren waren leeg enz.
In the new 'reality' we will be living in,nothing will be real and everything will be true-David A.McGowan
Why do some people not credit the origin of the quotes they use under their posts?- Tingo
Why do some people not credit the origin of the quotes they use under their posts?- Tingo
Weet ik niet - misschien geeft hij ook September Clues gelijk.quote:
[..]
Wat zou Orwell daarvan vinden?
In the new 'reality' we will be living in,nothing will be real and everything will be true-David A.McGowan
Why do some people not credit the origin of the quotes they use under their posts?- Tingo
Why do some people not credit the origin of the quotes they use under their posts?- Tingo
Als Alex Jones (A.J.) en David Icke niet zouden bestaan waren ze wel in het leven geroepen door de heersende elite. Ik denk overigens niet dat de elite A.J. en co aansturen, dat is helemaal niet nodig. Kijk maar naar hoe snel er werd beweerd dat de bomaanslagen in Boston een inside job waren. De trutherscene houdt zichzelf in stand en is al even onderhevig aan interne strijd als de Kerk. Er zijn zoveel tegenstrijdige theorieën in omloop die bovendien eenvoudig opzij te schuiven zijn vanwege het idiote karakter (WTC opgeblazen door atoombommen?quote:
[..]
[..]
Nee, over mensen als Alex Jones en David Icke. Ze bedoelen het zelf goed, alleen ze zijn gewoon puppets van de elite. Mensen die iets beginnen te begrijpen van de wereld gaan op onderzoek uit, komen vervolgens bij Alex of David uit omdat ze door de elite op het internet gepromoot worden, en krijgen zo de verkeerde info, de info die al lang door de filters van de elite zijn geweest. Hier gaat het dan ook fout, want die mensen die naar hen luisteren denken dat ze echt ''awake'' zijn, maar ze worden juist nog een keer gehersenspoeld. Ga vooral zelf op onderzoek uit en wees ruimdenkend, denk voor jezelf.
Het is de ultieme manifestatie van de wet van Poe:
quote:Poe's Law is an observation that it's difficult, if not impossible, to distinguish between parodies of religious or other fundamentalism and its genuine proponents, since they both seem equally insane. For example, some conservatives consider noted homophobe Fred Phelps to be so over-the-top that they argue he's a "deep cover liberal" trying to discredit more mainstream homophobes.
http://rationalwiki.org/wiki/Poe
Zo is het,ja.quote:
[..]
[..]
Nee, over mensen als Alex Jones en David Icke. Ze bedoelen het zelf goed, alleen ze zijn gewoon puppets van de elite. Mensen die iets beginnen te begrijpen van de wereld gaan op onderzoek uit, komen vervolgens bij Alex of David uit omdat ze door de elite op het internet gepromoot worden, en krijgen zo de verkeerde info, de info die al lang door de filters van de elite zijn geweest. Hier gaat het dan ook fout, want die mensen die naar hen luisteren denken dat ze echt ''awake'' zijn, maar ze worden juist nog een keer gehersenspoeld. Ga vooral zelf op onderzoek uit en wees ruimdenkend, denk voor jezelf.
In the new 'reality' we will be living in,nothing will be real and everything will be true-David A.McGowan
Why do some people not credit the origin of the quotes they use under their posts?- Tingo
Why do some people not credit the origin of the quotes they use under their posts?- Tingo
Judy Wood.quote:
Iemand een verklaring voor de spaghetti op deze brandweer auto?
[ afbeelding ]
Oh nee zeg!
Zij kan ook op t lijst van fakers.en afwijkers....met Willie Rodriguez,Richard Gage etc.
In the new 'reality' we will be living in,nothing will be real and everything will be true-David A.McGowan
Why do some people not credit the origin of the quotes they use under their posts?- Tingo
Why do some people not credit the origin of the quotes they use under their posts?- Tingo
wat is jouw verklaring dan?quote:
[..]
Judy Wood.
Oh nee zeg!
Zij kan ook op t lijst van fakers.en afwijkers....met Willie Rodriguez,Richard Gage etc.
Dat t waarschijnlijk is 'n foto expres gemaakt heel lang voor t 'dirty deed' om mensen te afwijken.quote:
Ik weet dat er heel goed mensen zijn in t Truth Movement.....maar t is echt heel jammer dat er is zo veel tijd wasted over red herring discussies.
Ik was heel teleurgesteld - echt.
In the new 'reality' we will be living in,nothing will be real and everything will be true-David A.McGowan
Why do some people not credit the origin of the quotes they use under their posts?- Tingo
Why do some people not credit the origin of the quotes they use under their posts?- Tingo
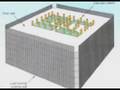
Na het zien van een gedeelte van Confronting the Evidence vond ik dit gedeelte erg interessant. De 47 core columns waren enigszins in een rechthoek verspreid vanaf het midden en niet beladen met materiaal wat hen goed kon laten branden, verhitten en verzwakken. Er waren zelfs liftschachten bij de core columns, die schijnbaar geen haard effect konden creëren. Hoe deze zo makkelijk hebben kunnen instorten, nadat er slechts enkelen door de vliegtuigcrashes waren beschadigd blijft een mysterie.
We must question the story logic of having an all-knowing all-powerful God, who creates faulty Humans, and then blames them for his own mistakes.
Het patent voor het "nanothermite device" ( http://www.google.com/patents/US5532449 ) bevat nergens het woord nano, het spreekt slechts over "finely divided". Maar dat terzijde.quote:
Hij doet alsof dit "device" iets is dat je kon inbouwen of plaatsen in het gebouw en dan activeren, waardoor de balken doorsmelten en hopla. In werkelijkheid is het patent een soort veiligere versie van een thermische lans, of stiller alternatief voor een slijpschijf, of voor een water cutter etc...
Dit is de manier waarop zo'n "device" gebruikt zou worden:quote:In detail, the present invention 101 is free of a potential fire because of the capability of controlling the heating, and does not produce any noise. Because of a good thermal efficiency, the present invention is applicable to both small-sized and large-sized concrete demolishing apparatus. The present invention also shows a high cutting capability and a low running cost of cutting.
The concrete cutter 102 is low in running cost of cutting, but produces a large amount of noise.
The thermite type lance 103 is high in cutting capability, but provides difficulty in controlling the heating, and has the danger of a potential fire.
The water jet 104 has a problem of having to dispose of the water used.
The thermal-stress break type plasma arc cutter 105 is poor in breaking efficiency, and hence requires a secondary breaking effort.
The melt type plasma arc cutter 106 is poor in thermal efficiency and high in running cost of cutting.

het enige verschil is dat hier de ijzeren lans opbrandt door er zuurstof door te pompen, in het patent wordt i.p. daarvan een gasstroom met thermietpoeder door de lans geblazen en aan het uiteinde ontstoken door een elektrische boog, wat het proces meer controleerbaar maakt omdat je de toevoer van de brandstof (het thermietpoeder tov het ijzer van de lans) beter kunt sturen. Zoals het patent zegt is het voordeel dat er minder kans op brand is, maar dat zou in het geval van het WTC niet uitmaken, en voor de rest is er geen wezenlijk verschil. Ik neem aan dat er geen zelfmoordenaars gebruikt werden, dus zouden er zowat 90 op afstand bediende lansen gebruikt zijn, elk op een robotarm, met gastank, thermiet poeder reservoir, menginrichting en regeling etc..
Dan lijken explosieve holle snijladingen me nog een meer discrete (onopvallende) oplossing.
En al de bedrijven die hij opnoemt die op één of andere manier in verband kunnen gebracht worden met thermiet research en die net op de getroffen verdiepingen gevestigd waren, hoe past dat in het plot? Als ze toevallig in een ander gebouw waren gevestigd dan had men dat aangevallen? Of had men al jaren op voorhand gepland en daarom de bedrijven daar gevestigd zodat men al het bewijsmateriaal, wat dat dan ook zou mogen zijn, kon vernietigen? Nogal een taktiek, we gaan het zo onopvallend mogelijk doen, dus plaatsen we de bureaus van de hoofrolspelers in de samenzwering precies daar waar de vliegtuigen inslaan, en we zorgen dat door toeval de personen in kwestie die dag niet op kantoor zijn zodat ze meteen voor de tv kunnen verschijnen om de vinger te wijzen naar al qaida...
[ Bericht 9% gewijzigd door meth1745 op 21-04-2013 12:15:29 ]
Het gedeelte van de core in de beschadigde verdiepingen was z'n isolatie kwijt; warmte stijgt, dat er geen luchtkanaal naar boven was betekent minder zuurstof, maar de warmte hoopt zich nog steeds op, de bovenste lucht/rooklaag bereikte temperaturen van 800 tot 1000 graden. Maakt niet uit dat er in de core zelf geen vuur aanwezig is, het zijn de hete gassen die de core verwarmen.quote:
Na het zien van een gedeelte van Confronting the Evidence vond ik dit gedeelte erg interessant. De 47 core columns waren enigszins in een rechthoek verspreid vanaf het midden en niet beladen met materiaal wat hen goed kon laten branden, verhitten en verzwakken. Er waren zelfs liftschachten bij de core columns, die schijnbaar geen haard effect konden creëren. Hoe deze zo makkelijk hebben kunnen instorten, nadat er slechts enkelen door de vliegtuigcrashes waren beschadigd blijft een mysterie.
De NIST simulaties voor WTC1 varieerden wat betreft de snelheid van het vliegtuig en de massa. case A (443 mph) en B (472 mph): Gebroken kolommen: 3 / 6 ; zware schade 3 / 3 ; moderate 3 / 4. lichte schade 1 / 5. Totaal aantal 47.
In case A, op verdiep 96 bereiken 7 vooral smalle kolommen temperaturen van 600° of meer, zestien tussen 300° en 600°, en 22, vooral de dikste kolommen blijven onder 300°.
Voor case B zie ik negen kolommen die 450° tot >600° halen, maar die figuur is niet helemaal duidelijk, zijn er enkele die grijs lijken, een kleur die niet in de legende voorkomt...
Case A werd verworpen op basis van de beelden van de uiteindelijke collapse.
NIST scenario voor WTC1:
impact, deel van load op noordzijde (7%) wordt via dakgebinte overgedragen op core, rest op nabijgelegen buitenkant; door de schade aan noordkant is er een lichte overhelling, zuidkant verliest deel van load (7%) die ook via dakgebinte aan core en west en oostkant wordt doorgegeven.
Expansie van de core door opwarming neemt meer van de buitenload over. De verdiepen zetten uit in horizontale richting, duwen naar buiten. Na verder opwarming beginnen de verdiepen door te hangen, struts knikken door, verdiepen trekken de buitenkolommen inwaarts.
Verdere opwarming van de core verzwakt het metaal, minder draagkracht, die kolommen worden in elkaar gedrukt (plastische vervorming), core krimpt, load komt via dakgebinte meer op de buitenkant te staan, tot de zuidkant inwaarts begint te buigen door de trekkracht van de doorhangende verdiepen.
Na 100 minuten is zowat 20% van core load overgedragen op de buitenkant: noord en zuid dragen nu 10% meer load, oost en west 25%. oost en west meer omdat ze rechter, stijver en minder beschadigd zijn dan N en Z.
De zuidkant kolommen worden onstabiel; door het buigen/knikken beginnen de verbindingen te falen. het knikken verspreidt zich over de hele zuidkant, deze kan geen load meer dragen, die wordt via de spanten en dakgebinte overgedragen op core en W en O kant.
Het deel van het gebouw boven de impactzone begint naar Z over te hellen, de O en W kolommen aan de zuidkant worden overbelast, en beginnen door te knikken, meer load komt op de core te staan, de core en de resterende buitenkolommen kunnen het gewicht niet dragen, en knikken ook, verbindingen tussen de kolomsegmenten breken, heel de boel zakt ineen.

Bedankt voor de info Meth. Ik heb het aandachtig gelezen, ik zal het nog wel een keer moeten lezen.
Edit: Heb je nog een makkelijk toegankelijke bron voor een leek?
Edit: Heb je nog een makkelijk toegankelijke bron voor een leek?
We must question the story logic of having an all-knowing all-powerful God, who creates faulty Humans, and then blames them for his own mistakes.
Hier een site met veel, docu's clips, audio en pdf files:
http://archive.org/detail(...)tWhatExactlyHappened
http://archive.org/detail(...)tWhatExactlyHappened
Euh, makkelijk toegankelijk weet ik niet, heb het uit het NIST rapport gehaald.quote:Op zondag 21 april 2013 18:55 schreef Being het volgende:
Bedankt voor de info Meth. Ik heb het aandachtig gelezen, ik zal het nog wel een keer moeten lezen.
Edit: Heb je nog een makkelijk toegankelijke bron voor een leek?
http://www.nist.gov/customcf/get_pdf.cfm?pub_id=909017
Er zijn ook een hoop draft reports (voordien verschenen), die bevatten meer details, appendices etc.. ook veel handgeschreven documenten ...
http://www.nist.gov/el/disasterstudies/wtc/wtc_draftreports.cfm
Maar andere bronnen weet ik niet zo meteen te noemen, misschien iemand anders die kan verder helpen?
Vind zelfs geen nederlandstalige site met een overzicht van technische termen gebruikt in dit soort constructies.. Geen idee wat de nederlandse termen zijn voor zaken als truss top chord, truss web diagonals, struts, gusset plates, stand-off plates, spandrels, spandrel splices etc.. (zijn wel duidelijk in het rapport, met de illustratie erbij). M'n (geërfde) technische Winkler Prins van 1953 helpt me ook niet verder (en die betrouw ik niet zo erg sinds ik erin las dat "diamant een zeer slechte warmtegeleider is"; het geleidt warmte 5.5 maal beter dan koper....
sorry, maar als je NIST als bron neemt, gaan je berekeningen niet goed zijn.quote:
[..]
Euh, makkelijk toegankelijk weet ik niet, heb het uit het NIST rapport gehaald.
http://www.nist.gov/customcf/get_pdf.cfm?pub_id=909017
Er zijn ook een hoop draft reports (voordien verschenen), die bevatten meer details, appendices etc.. ook veel handgeschreven documenten ...
http://www.nist.gov/el/disasterstudies/wtc/wtc_draftreports.cfm
Maar andere bronnen weet ik niet zo meteen te noemen, misschien iemand anders die kan verder helpen?
Vind zelfs geen nederlandstalige site met een overzicht van technische termen gebruikt in dit soort constructies.. Geen idee wat de nederlandse termen zijn voor zaken als truss top chord, truss web diagonals, struts, gusset plates, stand-off plates, spandrels, spandrel splices etc.. (zijn wel duidelijk in het rapport, met de illustratie erbij). M'n (geërfde) technische Winkler Prins van 1953 helpt me ook niet verder (en die betrouw ik niet zo erg sinds ik erin las dat "diamant een zeer slechte warmtegeleider is"; het geleidt warmte 5.5 maal beter dan koper....)
Mogelijk, maar voor de officiële versie lijkt het me de beste bron.quote:
[..]
sorry, maar als je NIST als bron neemt, gaan je berekeningen niet goed zijn.
Ik weet niet of deze video ooit gepost is, maar overduidelijk sequence van bommen die afgaan in WTC 7 op 8:35


slightly off-topic:betreffende Susan Lindauer (stem in begin van clip); die is aangeklaagd geweest voor werken in dienst van Saddam, maar was "mentally incompetent to stand trial". toen wilde men haar gedwongen behandelen met neuroleptica.quote:
Ik weet niet of deze video ooit gepost is, maar overduidelijk sequence van bommen die afgaan in WTC 7 op 8:35
Goed om te zien dat de rechter de psychologen en psychiaters het respect geeft dat ze verdienen:
http://www.scribd.com/doc(...)8-F-Supp-2d-558-2006quote:Susan Lindauer is charged in four counts with conspiring to act and acting as an unregistered agent of the government of Iraq, in particular the Iraq Intelligence Service ("IIS"), fromOctober 1999 until February 2004, and engaging in various forbidden financial transactionswith that government during that period, apparently in connection with her alleged role asagent of that government. At least a half dozen mental health professionals, including apsychologist and a psychiatrist retained by the defense, and several psychologists and psychiatrists employed, and one psychiatrist retained, by the government, have found hermentally incompetent to stand trial, due principally to delusions of grandiosity and paranoiathat make her unable to assist meaningfully in her own defense and understand the nature ofthe proceedings she faces. Defendant, but not her lawyer, has refused to accept thediagnosis and has refused to take psychotropic drugs that government physicians wish to administer in aid of rendering her competent to stand trial. The government has movedpursuant to Sell v. United States,
539 U.S. 166, 123 S.Ct. 2174, 156 L.Ed.2d 197 (2003)foran order compelling administration of such drugs. Lindauer, through and with the approval ofher lawyer, opposes the motion.
[..]
2.Evidence Bearing on Disputed Issue of Forced Medication
All the mental health professionals at the Carswell facility endorsed in their reports the idea of prescribing antipsychotic medication for defendant. Indeed, even Drs. Shadduck and Greg,
who hold Ph.D. degrees and accordingly are not, so far as I am aware, authorized to prescribe medication, nonetheless opined that "[a]ntipsychotic medications are the best treatment for symptoms of psychosis" (Shadduck Reports 12/13/05, 12/28/05 at 5) (see VasReport 12/19/05 at 2; Letter of William M. Pederson, M.D. to the Court, Jan. 19, 2006, at 1) Dr. Vas submitted the above-referenced two-page report, in which he concluded that it is medically necessary to treat defendant with antipsychotic medications, that they are"substantially likely" to render her competent, and that the side effects listed in his letter are rare and can be dealt with through "treatment strategies," and that in any event defendant does not to his knowledge suffer from any medical condition which would place her at substantial risk of developing any severe side effects. Dr. Vas also testified at the hearing, and did so with the same bland assurance and utter lack of substantiation. He stated in conclusory form his professional belief that "antipsychotics are medically necessary and appropriate and that, although there is a risk of various side effects, the risk of the side effects are rather rare and fairly easily managed" (5/4/06 Tr. 24), and specifically as to defendant, answered in the affirmative to the question, "[i]n your opinion, is involuntary administration of antipsychotic medication medically appropriate to treat Ms. Lindauer for her mental condition?" (Id.at 28) He recommended what are referred to as second generation or atypical antipsychotic medications that "are much more easily tolerated by patients, and we have some evidence that they have a less deleterious effect on cognition and help people think more rationally."
In the same broad fashion, he testified to experience with "people that . . . might complain of a side effect, and we try to alleviate side effects as much as we can and try to meet the treatment goals at the same time." (Id.at 25)
Similarly, and without elaboration, he testified that it was "extremely likely" that defendant would respond positively to antipsychotic medication, and added that "[t]here have been a few studies done that have been published in the literature which would indicate a restoration to competency that is above 80 percent, anywhere from 80 to 95 percent and that has included patients from various diagnostic categories and their response to particularly antipsychotic treatment." (Id.at 29
The government appears to have placed principal reliance on the testimony of its retained psychiatrist, Dr. Kleinman. He submitted an extensive initial report, cited above, that focused entirely on the diagnosis of defendant's condition. However, he submitted a later report that discussed treatment, and testified as well on the issue of forced antipsychotic medication. His second report described why he prefers his diagnosis to that of Dr. Goldstein, but stated also that even if defendant is diagnosed as suffering from delusional disorder, "second generation, i.e., `atypical', antipsychotic medication would reasonably likely—safely—help her." (Kleinman 4/7/06 Report at 10) Although the report supports that conclusion by quoting four studies that are optimistic as to the potential effectiveness of second generation antipsychotic medication in treating delusional disorder, all are anecdotal, which is to say none report on controlled studies. The most optimistic, dated in 1995, reports an overview of the literature that suggests "80.8% of patients show total or partial recovery" (id.at 15), but that conclusion is hemmed in with qualifications, as follows:
The authors are well aware that the outcome of this delusional disorder treatment overview is tentative. The existing literature has been investigated thoroughly, but its quality is extremely diverse, nomenclature is highly variable,and extended-case series are rare. The simplest details are often missing, suchas dosage schedules, side effects, duration of drug use, etc., as well as reasons for choosing or changing drugs. Duration of follow-up is extraordinarily variable.Another confounding factor in looking at outcome results with different treatments is that pimozide has generally become the first-choice treatment in recent years. Therefore, other neuroleptics tend to be employed in somewhat older studies. This may make their direct comparison even less reliable than otherwise
At the hearing, Dr. Kleinman came bearing a later report, published in February 2006, that reviewed the literature dating back to 1994 dealing with treatment of delusional disorder.(5/4/06 Tr. 79; GX 2) According to Dr. Kleinman, the new report concludes that the literature indicates "an effectiveness overall of various types of antipsychotic medication to be approaching 90 percent, in the high 80 percent." (Id.at 80) (emphasis added) The word"overall" here is significant, because Dr. Kleinman testified further as follows:
Q. And with respect to persecutory and grandiose types of delusion [the two types with which defendant is afflicted], what are the results as reported in the article?
A. Well, there is a total of 15 reported cases of persecutory delusions and there are a little bit more than 50 percent, eight [of] fifteen, are reported to be improved. None are reported to be recovered entirely, and there were no patients specifically with grandiose delusions. Moreover, Dr. Kleinman acknowledged a substantial ambiguity even in the "overall" figure,when he noted that the report showed elsewhere that a "positive response to medication treatment occurred in nearly 50 percent." (Id.at 81) He speculated that the apparent contradiction between the 50 percent and 90 percent figures could have occurred because at one point recovered and improved patients had been lumped together to generate the 90 percent statistic, but the author did not explain what was meant by "positive response" in nearly 50 percent of the cases. Dr. Kleinman conceded that this explanation was "not an entirely satisfactory one." (Id.) He offered for guidance also an article describing a single success in treating delusional disorder with Risperidone (GX 3), a second generation or atypical antipsychotic medication (5/4/06 Tr. at 83-84). However, the last sentence of the conclusion in that article reads as follows: "A controlled clinical trial of Risperidone in the treatment of patients with delusional disorder is warranted." (Id.at 85) Dr. Kleinman explained the absence of evidence from controlled clinical studies by pointing out that delusional disorders are generally rarer than schizophrenic disorders, and accordingly it is difficult to obtain data with respect to delusional disorders and resources are directed more at the schizophrenic disorders. (Id.at 86) Later, he agreed that controlled studies are a"more desirable source of data for making treatment decisions." (Id.at 90) Despite the absence of controlled studies, and the "critical eye" with which case studies must be approached, he answered "Yes" to inquiries as to whether "involuntary administration of antipsychotic medication [is] medically appropriate to treat Ms. Lindauer's symptoms" and whether such treatment would "improve Ms. Lindauer's chances to be restored to mental competency to stand trial." (Id.at 87)That was as strong an endorsement as he gave to involuntary medication.
It bears mention here that initially, when he was not responding to leading questions, he testified simply that "there is only one type of treatment that holds any promise of diminishing . . . the psychotic disorder not otherwise specified and that is antipsychotic medicine." (5/4/06 Tr. 63) That testimony says nothing about the likelihood that such treatment would succeed, but only that it is the sole treatment that could succeed in treating what he characterized as "a condition very much worthy of treatment." (Id.at 89) Dr. Goldstein, defendant's retained psychiatrist, explained his preference for the diagnosis of delusional disorder, mixed type over psychotic disorder not otherwise specified (5/9/06 Tr. 6,32-33), but readily noted that from the standpoint of treatment, the two defined "a distinction without a difference." (Id.at 28)He reviewed the weaknesses of the paper Dr. Kleinman had brought to the hearing, GX 2,including not only that there were no controlled studies but also that, there aren't many articles where someone says I treated six patients with this illness and none of them got better. Those kind of papers are generally not published. So there's a kind of skewing of the literature towards only writing about things where you have a favorable outcome.
Dr. Kleinman spoke principally of the likely effect of unsuccessful treatment on defendant's relationship with her lawyer, and said it was by no means certain that relationship would deteriorate because the relationship continued intact at the time of the hearing (5/4/06 Tr. at 68), although he conceded that an"extreme" reaction would be for her to "become very angry at him and reject him."
As to physical side effects, Dr. Kleinman agreed that certain of such side effects were possible, but emphasized that monitoring and screening of patients could mitigate or prevent the onset of such symptoms (5/4/06 Tr. 71-73, 92), although he agreed that a physician charged with monitoring a large number of patients would have a harder time monitoring each patient effectively (id.at 92). Dr. Goldstein relied on a pharmacology text (DX D) to project various percentages of physical side effects, principally including EPS, or extrapyramidal syndrome, which encompasses various degrees of muscular disorder and pseudo-Parkinsonism, with tremors, rigidity, and other involuntary muscular phenomena.(5/9/06 Tr. at 21) Such phenomena became more likely as the dosage increased, reaching 25 percent for Risperidone at a 16 mg level (DX D), which he said is considered a high incidence. (5/9/06 Tr. at 22;see also DX C) He testified that the recorded incidence of neurologic malignant syndrome, or NMS, in patients taking these medications is 2 percent,with 20 percent mortality in patients suffering NMS, a death rate of 4 per 1,000. (4/9/06 Tr.24)
http://en.wikipedia.org/wiki/Susan_Lindauerquote:On January 16, 2009, the government decided to not continue with the prosecution saying "prosecuting Lindauer would no longer be in the interests of justice.